Cervical fractures are common in the geriatric population, but we pay less attention to those with minimal trauma.
The Geriatric Fall
A 72-year-old man is brought in by EMS after a fall. When he arrives, he is supine and immobilized on a backboard with a c-collar in place. He states he was walking from the kitchen into the living room and tripped on the transition. His only complaint is minor neck pain. There was no loss of consciousness, nausea, vomiting, or sensory deficits. His vital signs are stable.
Suddenly, a long list of questions comes to mind: is the neck pain from an injury, or from his cervical collar? How likely is a cervical spine (c-spine) fracture? Can you apply clinical decision rules in this geriatric patient? Are there other injuries that are important to consider in this population? What risks does immobilization have in the geriatric population?
How likely is a cervical fracture in the geriatric trauma patient?
Ground level falls are typically considered a minor trauma, but in the geriatric patient, that 9.8m/s2 acceleration is enough to cause significant blunt trauma injuries (figure 1 below). Over half of the geriatric cervical fractures are caused by low-impact or a ground level fall [1]. Approximately 19% of all cervical fractures are in the geriatric population. Compared to a younger population, the geriatric trauma patient is twice as likely to have a c-spine injury from similar trauma [2].

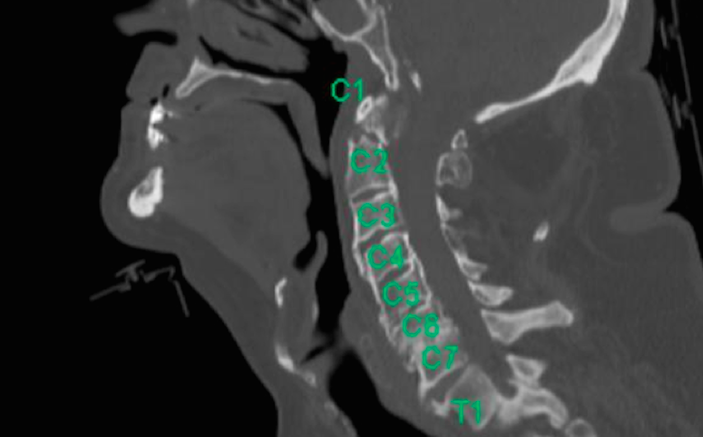
The mobility of the c-spine in an older adult is also different. In a younger trauma patient, cervical fractures are most common in the lower cervical spine—C6 or C7, but in the geriatric population a fracture is much more likely to occur in C1 or C2, with over 50% of fractures in C2 [3]. This limits the reliability of c-spine palpation in detecting these fractures, and increases the morbidity and mortality of these injuries. The one-year mortality of a geriatric patient after a cervical fracture is approximately 40%, higher than mortality after hip fracture [4,5].
Do clinical c-spine screening criteria apply to the geriatric trauma patient?
The two most commonly used clinical decision rules to assess the need for cervical imaging in the trauma patient is the Canadian C-Spine Criteria and the NEXUS criteria. The Canadian criteria recommend a CT c-spine for any patient ≥65 years old [6]. The NEXUS criteria are not as clear [2]. The original NEXUS study included a sufficient number of geriatric patients and a geriatric subgroup analysis showed 100% sensitivity for clinically significant injury in the original study population. However, many clinicians do not apply this rule because of the prevalence of fractures in geriatric patients with minimal trauma or symptoms [7]. A study of 320 older adults with blunt trauma found that NEXUS had a sensitivity of 65.9% and a PPV of 19.3%, which is inadequate to rule out a c-spine fracture [8]. This was a cohort of severe blunt trauma patients, so it is possible that a low clinical suspicion based on mechanism plus NEXUS is enough to rule out fractures. Another team looked at only those older adults with low energy mechanisms of trauma, such as ground-level falls. NEXUS was again inadequate as only 45% of older adults with documented c-spine fractures had neck tenderness upon presentation [9]. Intoxication might explain the lack of cervical spine tenderness in elderly patients with cervical fractures, but only 3% of older adults with c-spine fractures have alcohol in their system at the time of their fall as compared to 53% of younger trauma patients with c-spine fractures [1]. This removes intoxication and distracting injuries from the equation. Do older adults who are alert, asymptomatic, and have a normal neurologic exam require imaging despite no c-spine tenderness?
A series of 274 older adults who fit these criteria found that 3% had c-spine fractures despite being entirely asymptomatic [10]. Therefore, clinically clearing these patients will still result in a few missed fractures.7 Regardless of which clinical criteria you use to screen an older adult with a fall and head or neck trauma, it will miss a fracture at some point. There is a high enough percentage of initially asymptomatic patients to lead to missed diagnoses. Therefore, I apply the rule of common sense. Almost all older adults with a fall should have a CT C-spine to evaluate for fracture. If the patient is alert, has no cognitive impairment, is asymptomatic, and is capable of returning to the ED easily if they develop problems, I will have a conversation about risks and benefits. I usually quote a 5% miss rate instead of 3%, because 3% seems to be too clinical and distracting a number to understand for many patients.
What other injuries are important to consider in geriatric cervical trauma?
Many cervical fractures occur as isolated injuries in the geriatric population. There are also other associated injuries that can be of concern (figure 2 below). Approximately 20% of patients who have a spinal column fracture have an additional non-contiguous fracture. While non-contiguous fractures are most common in high-velocity trauma, they should be considered in any geriatric trauma patient with a c-spine fracture [12]. Intracranial injuries are the most common concurrent injury found in 6% of older adults with c-spine fractures [1]. Vertebral artery injuries may also be associated with c-spine fractures. In one retrospective study, 17% of the patients who were screened for vertebral artery injury were found to have an injury and these were associated with high-risk fractures [13].

What about c-spine immobilization?
C-spine immobilization for older adults is an area of controversy, and may cause more harm than good [14]. Older adults experience pain from cervical collars due to underlying osteoarthritis, respiratory difficulties from immobilization, and delirium from the restriction and discomfort of the collar [15]. Often, distracting injuries in the trauma patient are considered an indication for initial cervical immobilization. However, further research needs to be conducted in order to better guide initial immobilization because less than 2% of patients with a hip fracture — a clear distracting injury — may have an associated cervical spine fracture [11]. Some data suggests that a distracting injury above the clavicle is of higher association with spinal fractures. Cervical immobilization is probably not necessary if the patient is alert, not agitated or delirious, and able to control his or her own neck movements well with transfers. In the prehospital situation however, often a lack of a c-spine collar may make ED providers feel that the c-spine has already been cleared, which is not the case. If a collar is placed, attention to quick removal when the c-spine is cleared is very important. More research is needed into the pros and cons of immobilization.
Once a c-spine fracture is diagnosed, treatment options can vary. There are three basic treatment options: rigid collar without fracture reduction, halo cast with reduction of a fracture, and surgery. There is significant debate as to the best approach. One literature review found that there is no significant difference between the treatment options in morbidity and mortality16 while another found that in well-selected patients, surgical treatment reduced the risk of short-term and long-term mortality [17]. One possible approach for initially asymptomatic patients without cord compression is bracing with serial x-rays as surgery may be delayed without significant effect on the overall clinical outcome [18].
The Bottom Line
High cervical fractures are much more common in the geriatric trauma population, even with minimal trauma, and our normal clinical decision screening rules are much less sensitive in these patients. Although many of these fractures are isolated, there are also important associated injuries that need to be considered. CT should be the first imaging used to evaluate for c-spine injury in these older patients, and while initial immobilization is important, we should be quick to liberate patients with negative imaging from cervical collars and to involve a spine surgeon with positive imaging.
REFERENCES
- Wang H, Coppola M, Robinson RD, et al. Geriatric Trauma Patients With Cervical Spine Fractures due to Ground Level Fall: Five Years Experience in a Level One Trauma Center. J Clin Med Res. 2013;5(2):75-83.
- Touger M, Gennis P, Nathanson N, et al. Validity of a decision rule to reduce cervical spine radiography in elderly patients with blunt trauma. Ann Emerg Med. 2002;40(3):287-293.
- Morrison J, Jeanmonod R. Imaging in the NEXUS-negative patient: when we break the rule. Am J Emerg Med. 2014;32(1):67-70.
- Cooper Z, Mitchell SL, Lipsitz S, et al. Mortality and Readmission After Cervical Fracture from a Fall in Older Adults: Comparison with Hip Fracture Using National Medicare Data. J Am Geriatr Soc. 2015;63(10):2036-2042.
- Venkatesan M, Northover JR, Wild JB, et al. Survival analysis of elderly patients with a fracture of the odontoid peg. Bone Joint J. 2014;96-B(1):88-93.
- Stiell IG, Wells GA, Vandemheen KL, et al. The Canadian C-spine rule for radiography in alert and stable trauma patients. JAMA. 2001;286(15):1841-1848.
- Collins NC, McKenzie JV. The NEXUS criteria: do they stand the test of time? Eur J Emerg Med. 2013;20(1):58-60.
- Goode T, Young A, Wilson SP, Katzen J, Wolfe LG, Duane TM. Evaluation of cervical spine fracture in the elderly: can we trust our physical examination? Am Surg. 2014;80(2):182-184.
- Schrag SP, Toedter LJ, McQuay N, Jr. Cervical spine fractures in geriatric blunt trauma patients with low-energy mechanism: are clinical predictors adequate? Am J Surg. 2008;195(2):170-173.
- Ong AW, Rodriguez A, Kelly R, Cortes V, Protetch J, Daffner RH. Detection of cervical spine injuries in alert, asymptomatic geriatric blunt trauma patients: who benefits from radiologic imaging? Am Surg. 2006;72(9):773-776; discussion 776-777.
- Boland LL, Satterlee PA, Jansen PR. Cervical spine fractures in elderly patients with hip fracture after low-level fall: an opportunity to refine prehospital spinal immobilization guidelines? Prehosp Disaster Med. 2014;29(1):96-99.
- Nelson DW, Martin MJ, Martin ND, Beekley A. Evaluation of the risk of noncontiguous fractures of the spine in blunt trauma. J Trauma Acute Care Surg. 2013;75(1):135-139.
- Lebl DR, Bono CM, Velmahos G, Metkar U, Nguyen J, Harris MB. Vertebral artery injury associated with blunt cervical spine trauma: a multivariate regression analysis. Spine (Phila Pa 1976). 2013;38(16):1352-1361.
- Oteir AO, Smith K, Stoelwinder JU, Middleton J, Jennings PA. Should suspected cervical spinal cord injury be immobilised?: a systematic review. Injury. 2015;46(4):528-535.
- Moran C, Kipen E, Chan P, et al. Understanding post-hospital morbidity associated with immobilisation of cervical spine fractures in older people using geriatric medicine assessment techniques: A pilot study. Injury. 2013;44(12):1838-1842.
- Delcourt T, Begue T, Saintyves G, Mebtouche N, Cottin P. Management of upper cervical spine fractures in elderly patients: current trends and outcomes. Injury. 2015;46 Suppl 1:S24-27.
- Schroeder GD, Kepler CK, Kurd MF, et al. A Systematic Review of the Treatment of Geriatric Type II Odontoid Fractures. Neurosurgery. 2015;77 Suppl 4:S6-14.
- Momin E, Harsh V, Fridley J, Winnegan L, Omeis I. Reliability of treating asymptomatic traumatic type II dens fractures in patients over age 80: A retrospective series. Journal of craniovertebral junction & spine. 2015;6(4):166-172.
1 Comment
Great review. Especially the 3% fracture rate in asymptomatic patients. Thanks for the review.