



 Research shows that early goal-directed therapy is improving survival rates for sepsis patients.
Research shows that early goal-directed therapy is improving survival rates for sepsis patients.
There is an estimated 750,000 cases of severe sepsis per year in the U.S. With our aging population and strengthening pathogens, these numbers are expected to double in the next 25-30 years, making sepsis an even more widely prevalent and devastating disease. Of all these cases, two-thirds present through the ED with an average ED LOS of 5 hours. Prior to Early Goal-Directed Therapy (EGDT), mortality estimates for sepsis have ranged as high as 56%. Sepsis occupies the largest growth in health care costs of the national bill from 1997-2005 and represents the 4th largest recipient of Medicare and Medicaid expenditures for hospitalized patients.

As the science currently stands, EGDT via an “invasive” approach has been proven and externally validated with similar mortality reductions (15-20%) in multiple studies comprising over 6,000 patients. The socioeconomic benefit of EGDT has repeatedly shown an average of a 20% reduction in sepsis related costs. This benefit exceeds that of other acute interventions such as thrombolytics for ST elevation MI (3-5% absolute mortality reduction). Given that nearly two-thirds of severely septic patients present through the ED, can EPs as resuscitation experts apply EGDT early in the patient’s presentation? Will EDs support their nursing staff and physicians in this effort? The answers are yes, and maybe.
Overcoming Practice Challenges
A 2004 national survey found that only 10% of EDs were routinely performing EGDT. By 2006 that number was increased to 45%. EGDT represents an enormous breakthrough in sepsis management that significantly impacts patient mortality and has been endorsed nationally and internationally via the Surviving Sepsis Campaign. Third party payors and insurance companies are incentivising hospitals with pay for performance for high risk diseases such as sepsis. Despite the push for practice change, why aren’t EDs and EPs performing it as much?
Despite well documented benefits and endorsement by international awareness campaigns, many EDs are still unaware of the benefits of this aggressive approach to sepsis and related shock. Why? Information overload and inadequate time may preclude practicing clinicians from in-depth familiarization with current research findings. What to do? Some of the strategies for staying abreast of EGDT literature include becoming familiar with appraisals, such as ACEP Clinical Guidelines, Cochrane, etc… Even more up to date information can be obtained by setting up automatic email notifications of clinically relevant evidence via topic specific parameters through individual journals or literature search engines. The Surviving Sepsis Campaign (survivingsepsis.org) and Institute for Healthcare Improvement (www.ihi.org) websites both contain useful references and resources for developing an EGDT protocol at both the institutional and provider level.
Acceptance
Despite EGDT being adopted as standard of care by multiple authorities, a 2006 survey found 32% of EDs were planning an EGDT protocol while 23% reported neither using nor planning an EGDT protocol. The reason given by some for this reluctance to acceptance is the traditional practice of delaying invasive monitoring to ICU admission. Others resist adoption of EGDT due to contradictory personal experience or skepticism of study results. A recent national survey found that 16% of EPs report a “lack of agreement with the EGDT protocol.” Despite this resistance from a minority the greater barrier to acceptance seems to be in whether the protocol is practical.
Applicable
Despite clear enrollment criteria for severely septic and septic shock patients, some EPs resist applying EGDT to their patients thinking that the study patients were somehow different from their patients. Are my patients older or sicker and less likely to benefit? Are my patients less sick and thus, less in need of aggressive monitoring? What about the patient that “looks good” with a lactate of >4? This notion has been disproven as others have validated similar mortality and illness severity with this screening criteria.
The scenario of “looking good/normotensive” despite a lactate >4 and being uncertain if they may benefit from a central line and EGDT is slightly more difficult. The majority of studies showing a mean 20% +/- 13% absolute mortality reduction from EGDT have used the same inclusion criteria as the original trial and combined results of septic patients with lactate ≥4.0 mmol/L and patients with persistent hypotension making it harder to tease out the severe sepsis (lactate >4) groups. Despite this, the lactate>4 group still showed a trend toward mortality reduction with EGDT.

Able
Overall most institutions that have successfully instituted EGDT can point to a physician champion that advocated for the resources needed to follow this protocol. Granted it is impossible to do without measuring a CVP or ScvO2 and these obviously need to be acquired or else EGDT will not happen. But once the ED acquires the appropriate equipment, department-wide training initiatives and nursing support are needed to educate physicians and nurses on EGDT endpoints. Some EDs train their nurses to monitor CVP and ScvO2 and to alert physicians when goals are not being met thereby freeing up physicians from hands-on bedside care.
Action
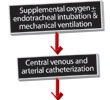
Standing order sets for severe sepsis and septic shock can be tailored for specific individual institutions (i.e. formulary medication, labs, monitoring, responsibilities). For instance, some patients use continuous ScvO2 monitoring while others test spot blood gasses from the central line for oxygen saturation. Regardless of the protocol, the core EGDT focus should remain on optimizing the MAP, CVP, and ScvO2.
Summary
The majority of severely septic and septic shock patients present through the ED with a short term mortality of 30-60% if treated without EGDT. Sepsis is an expensive disease process that already occupies a sizable portion of national healthcare costs, and it is anticipated to worsen in coming years. Multiple studies have shown that the survival rate can be improved (7-33% absolute mortality reduction) with a feasible and cost-effective means of treatment in the form of EGDT (Fig.1). EPs as resuscitation experts have the background and skill set to initiate management and stabilization of this critically ill patient population. However, individual provider and institutional barriers should be anticipated when attempting to set up or maintain an EGDT pathway.
Authors:
Chris Holthaus, M.D.
Chief Resident 2007-2008
Washington University Emergency Medicine Residency
Barnes-Jewish/St. Louis Children’s Hospital
Jeffrey Green, M.D.
Assistant Residency Director
Department of Emergency Medicine
New York Hospital Queens
Peer Reviewed:
Emanuel P. Rivers, MD, MPH, IOM
Vice Chairman and Director of Research,
Department of Emergency Medicine
Senior Staff Attending, Emergency Medicine and Critical Care
Henry Ford Hospital, Detroit Michigan
Institute of Medicine, National Academies