



Treating fractures of the radial and ulnar shaft
Introduction
The forearm is often seen as a static structure, when in reality, the complex nature of pronation and supination requires dynamic articulations independent of wrist movements and elbow. These movement are functionally as important or perhaps more important to essential activities of daily living.
The injuries we will focus on include isolated injuries of the radius and ulna, fracture dislocations of the radius and ulna and both bone forearm fractures. Distal radius fractures are discussed at length independently in a previous EPM article.

Anatomy
The forearm should be conceptualized as a ring not unlike the pelvis. The radius and ulna are bound by complex articulations distally at the distal radial-ulnar joint (DRUJ) and proximally by the radial head and the proximal radial ulnar joint (PRUJ). These articulations are responsible for pronation and supination.
It can been argued that the actions of pronation and supination are functionally more important for normal activities of daily living then wrist flexion and extension. Consider how often pronation and supination are performed in actions we take for granted: opening a door, turning a key, typing at a computer, carrying a plate of food. All of this actions can be affected by injuries to the PRUJ and DRUJ.
Because of the ring like anatomy, injuries in one location tend to result in ligamentous disruption or fracture elsewhere. This usually manifests as a fracture or dislocation the other forearm bone, or dislocation of the DRUJ or PRUJ. Often times the manifestation of a ligamentous injury is shortening of one bone relative to the other. The rare exception is with direct force with focal trauma to the ulna in which the remaining anatomy may be spared.

Ulnar Injuries
Night stick Injuries
The most straight forward injury to the forearm occurs when the ulna receives a focal and direct blow mid-shaft. These “Nightstick” Injuries are typically the result of a blocked assault. The ulnar shaft fractures with no significant shortening, displacement or angulation. The injury can be managed in a long forearm ulnar gutter splint for 7-10 days. They are often converted to a functional brace following initial splinting to allow early range of motion but this can vary depending on the orthopedist.
Some nightstick injuries will result in significant angulation or displacement. When isolated ulnar shaft fractures demonstrate more then 10 degrees of angulation or 50% displacement orthopedic consultation and open reduction is required.

Monteggia Fractures
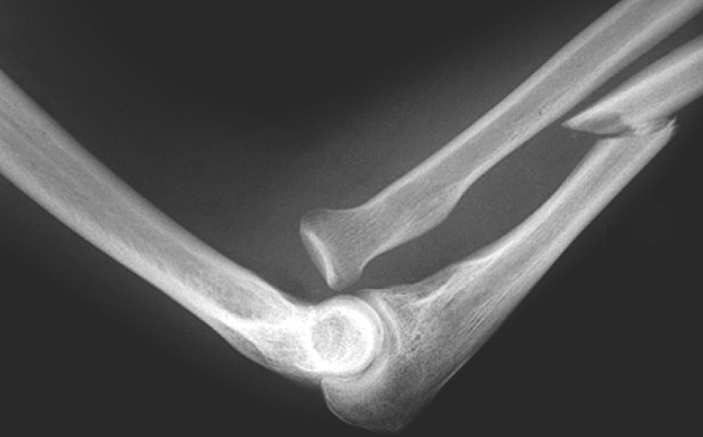
These unique injuries (pictured at the top of the article) are actually fracture dislocations involving the ulna and the PRUJ. The characteristic pattern involves a fracture of the proximal third of the ulna and a dislocation of the radial head. The dislocation can vary depending on the angulation of the proximal ulnar fragment. Anterior dislocations of the radial head are most common but posterior and lateral dislocations can also occur. Because the mechanism typically involves substantial force, the displacement of the proximal ulna simultaneously disrupts the annular ligament resulting in migration of the radial head. These injuries are not radiographically subtle and invariably require open reduction and internal fixation.

Radius fractures
As already mentioned, distal radius fractures are considered in an independent discussion and a previous article. For purposes here we will focus on Galleazzi fractures and isolated fractures of the proximal two thirds of the radius.
Isolated fractures of the proximal two thirds of the radius typically result from direct blow, not unlike nightstick fractures. If the fracture pattern is entirely non-displaced the can be managed with immobilization alone. Unfortunately even minimal displacement is poorly tolerated and will require open reduction and internal fixation.
Galleazzi fractures are unique in that they occur at the junction of the middle and distal third of the radius and are associated with disruption of the distal radial ulnar joint. Typically the displacement and shortening of the distal fragment causes the disruption in the articulation at the distal radial ulnar joint. Given the complexity of the fracture pattern and the associated DRUJ disruption, these fractures always require surgery with open reduction and internal fixation.

Both Bone Forearm Fractures
These injuries are far more common in pediatric patients then adults. Young pediatric management differs in that many younger patients are effectively managed with closed reduction and immobilization. The reduction can be intimidating. It is not uncommon that one of the two fractures is incomplete. This makes simple reduction extremely difficult. Efforts to simply reverse the mechanism often fail. These fractures emphasize the importance of recreating the mechanism of injury before reversing it. Intuitively it can be unsettling to worsen the deformity as part of the reduction maneuver but it is necessary for two reasons. First, as with many fractures, recreating the mechanism by exaggerating the deformity may be the only way to unlock periosteum that has become trapped in the fracture site. Second, recreating the injury may be necessary to complete the incomplete fracture and ultimately obstinate appropriate alignment. Again, this can procedure can be unsettling. The prospect “breaking” the incomplete fracture while exaggerating the deformity seems counterintuitive and perhaps intimidating but it is often necessary. Clear communication with parents is paramount especially if you opt to allow them to stay in the treatment room during the procedure. Splinting requires a double sugar tong for appropriate stabilization. Given the force typically required in reduction, care should be taken to allow for swelling and parents should be given strict instructions to monitor for change in colored the digits or other signs that the splint is too tight.

In older children nearing the closure of their growth plates a unique operative intervention may be considered by the orthopedist. Flexible nails, a type of intramedullary fixation that can be placed making very small incisions are effective in maintaining reduction and minimizing deformity in this unique population. They do not require interlocking screws and they are easily removed. Over the past decade orthopedics its have become more aggressive in using flexible nails in younger patients. Be sure to communicate with your on call,orthopedic at to clarify their intentions.
Both bone forearm fractures in adults always mandate open reduction and internal fixation. Closed reduction may be warranted in the emergency department if the deformity is so severe that there is skin tenting with impending conversion to an open fracture or if there is neuro-vascular compromise. Closed reduction is almost never the definitive treatment.

Summary
Injuries to the shaft of the ulna or radius rarely occur in isolation. The exceptions being isolated nightstick fractures of the mid shaft of the ulna resulting from a direct blow, and isolated injuries to the proximal radius that do not disrupt the radial head proximally or the DRUJ distally. Night stick fractures may require surgery if significant displacement occurs. Isolated proximal radial shaft fractures require surgery if even very little displacement is noted.
The remaining fractures discussed all involve associated injuries to various articulations critical to the dynamic function of the upper extremity. Monteggia fractures involve the proximal ulna have associated radial head dislocations and require surgery. Galeazzi fractures involve the junction of the middle and distal radius and have associated distal radial ulnar joint disruptions. Galeazzi fracture-dislocations also require surgical intervention.
Considering the dynamic role of the DRUJ and the PRUJ in the functionally essential activities of pronation and supination, injuries involving these structures must be identified and addressed by the ED physician.
Pearl: Dial M for Monteggia
I remember the difference between Monteggia fractures and Galeazzi fractures using a simple but effective visual association. Most X-rays of the elbow show the elbow bent at 90 degrees. That bend reminds me of the letter “M”, so the fracture dislocation near the elbow (proximal ulna and radial head dislocation) is the “M”onteggia fracture. By exclusion, distal injuries (radius at the junction of the middle and distal third with resulting DRUJ injury) must be the Galeazzi fractures.