A 16-year-old female has shortness of breath during dance class, but it’s much more than an anxiety attack
As you make your way into work on this sweltering summer day, your mind begins to think through all of the possible patients you may be called upon to treat. Anything may come through those ED doors. STEMI? Mesenteric ischemia? Ankle sprain? Heat stroke?
You walk over to your computer as the EMS patch phone squawks to life: “16 year-old female, history of anxiety, having shortness of breath during dance class. She looks like she is having an anxiety attack. Do we have permission to give 1 mg of Ativan? Vitals are: HR 120, RR 60, O2 sats 40%, BP 100/64. I think our sat monitor is broken. Over.”
Given the constellation of vital signs and the patient’s chief complaint, you think to yourself that there is no way this is mere anxiety. You quickly deny the pre-hospital request for Ativan and recommend that they expedite their arrival with lights and sirens.
When the EMS crew arrives with your patient. They have wheeled in a young, thin female sitting upright in the gurney, breathing at least 60 times per minute. You think to yourself, “This is definitely not an anxiety attack.” As the gurney is being wheeled down the hallway, you catch a glimpse of the cardiac monitor. It looks like sinus tachycardia at about 120 bpm. Just then, your patient’s breathing becomes more and more labored. She looks you right in the eye, and you register the fear in her young, innocent face. Almost instantaneously, she stops breathing. You instinctively check for radial and carotid pulses simultaneously. Nothing. “Start chest compressions now!” you order, as your team maneuvers the gurney into one of your resuscitation bays.
Following a successful intubation, your chief resident administered epinephrine, sodium bicarb, calcium chloride, and IV fluids as chest compressions were continued without interruption. Your team proceeds with the resuscitation, and you start your CORE scan with the ultrasound machine.
“Bag the patient a few times for me please.” You glance at the trachea and note that the ET tube is in place on ultrasound and then direct your attention to the lungs bilaterally. There is good lung sliding on ultrasound and you note a normal number of comet tails in the interspaces you scan through. There are no pleural effusions and there is normal diaphragm movement bilaterally with bagging.

Figure 1: ECG with S1Q3T3 and severe strain pattern in V1-V3
After a few rounds of epinephrine and good perfusion with chest compressions, your patient regains a faint but palpable pulse. As an epi drip is being started for her persistent hypotension, you pause your CORE scan long enough for an EKG to be obtained (Image 1).
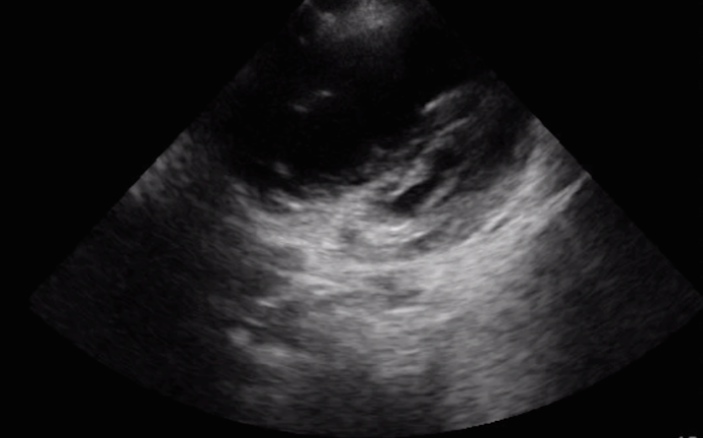
Continuing on with the CORE scan, you assess the patient’s heart. Image 2 is the parasternal short axis view you obtain. Image 3 is the apical 4-chamber view you see.

Figure 2: Parasternal long axis view of the heart with the indicator directed towards the patient’s left shoulder.

Figure 3: Apical 4-chamber view of the heart with the indicator directed towards the patient’s axilla.
What do you see on ultrasound? What should your next steps be in this patient’s resuscitation? Look closely. What do you see in the ultrasound images?
Based on the ultrasound findings and the patient’s clinical picture, you quickly recognize that your patient may be suffering from the effects of a massive pulmonary embolus. The patient’s parasternal short axis view of her heart and apical 4-chamber view of her heart demonstrate a large, dilated right ventricle and small, compressed left ventricle (Images 4 & 5).

Figure 4: Parasternal short axis view of the heart showing a dilated right ventricle (RV) left shoulder.

Figure 5: Apical 4-chamber view of the heart showing a dilated right ventricle (RV) that is larger than the adjacent left ventricle (LV).
You continue with the CORE scan and note that the patient’s IVC is dilated and that it is not really moving with bagging, but she has a normal aorta and no intra-abdominal free fluid. Without warning, your patient loses her pulse again and your chief resident asks for chest compressions to be initiated.
This is a critical juncture and everyone in the room knows it. Your chief resident looks to you for guidance, and you steadily say “What do you want to do now?” Sensing your support and agreement, she asks for the ED pharmacist to draw up tPA and you decide to push 50 mg given her size and continue with compressions to circulate the thrombolytic.
With a heavy heart, you tell the PICU team the story as your chief resident updates mom and brings her in to see her daughter. The PICU team discusses the prognosis with mom and together they decide to continue aggressive treatment and resuscitation. The patient is started on a peri-arrest cooling protocol for 48 hours and a tPA infusion is continued in the PICU.
A few weeks go by, and you finally find the time to follow up on your patient. The PICU team updates you that the patient continued to improve, and she underwent an MRI of her brain that showed multiple small infarcts, but no large disruption. Her neurological exam continued to improve, and she was eventually successfully extubated and transferred to a rehabilitation center.
You show up to work, months later, ready again to treat and care for anything that comes in your door. Surprised, you find yourself looking at a beautiful card sitting at your desk. Your 16 year-old patient made a full recovery and is requesting your presence at her upcoming dance recital. Your face lights up with a magnificent smile and you think to yourself, “It is definitely time to dance…”
Pearls & Pitfalls For Using Ultrasound During the Assessment of a Patient in Acute Respiratory Distress
Point-of-care ultrasound can provide invaluable information during the assessment of patients presenting in respiratory distress. Ultrasound can be performed rapidly and simultaneously during other resuscitative interventions at the patient’s bedside, and repeated as the patient’s clinical status changes.
The CORE scan (Comprehensive Overview of Resuscitative Efforts) can help guide and direct your resuscitative efforts while providing useful data during the evaluation of critical patients.
When caring for a patient that presents with cardiopulmonary arrest, evaluate the lungs and heart immediately with ultrasound to help identify rapidly reversible causes (e.g. tension PTX or hydrothorax, pericardial effusion and tamponade, acutely dilated RV from massive pulmonary embolus, etc.)
If you see an acutely dilated RV on ultrasound in a patient who presents with hypoxia, tachypnea, tachycardia, and hypotension, you should strongly consider the diagnosis of a massive pulmonary embolism.
It is rare to actually visualize a clot in the right side of the heart or in the IVC on ultrasound. It is more common to see the upstream effects of the massive pulmonary embolus as it causes acute RV dilation and IVC distension while it is blocking off circulation through the pulmonary arteries.
Other sonographic findings which support the diagnosis of an acute, large pulmonary embolism include: RV systolic dysfunction, flattening of the intraventricular septum or bowing of the septum towards the LV, IVC dilation without inspiratory collapse or variability, or evidence of a DVT on compression ultrasound of the upper or lower extremities.
In an unstable patient with a clinical picture that is suggestive of a massive pulmonary embolism, the ultrasound findings described above may guide the decision to administer thrombolytics or have the patient undergo an acute thrombectomy, or even ECMO, per your institution’s guidelines and policies.
There is no substitute for clinical experience and hands-on practice with point-of-care, bedside ultrasound. Practice, practice, practice.