
Ultrasound can succeed in mobilizing a surgeon when exam and labs fail to impress.
You are working a Sunday morning fast track shift. Your first patient is a 72-year-old male with a history of DM and HTN who came to the ED for right hand pain and swelling after being scratched deeply on the dorsum of the hand four days ago by his daughter’s cat. He made an appointment to see his doctor but didn’t want to wait until tomorrow to be seen because in the past two days he has noticed a gradually progressive inability to extend his middle three fingers. He denies any fever or other complaints
Vital signs are normal. There is not even a low-grade temperature (it is 98.2). Physical exam is basically normal except for the right hand. On inspection, there is an unimpressive amount of swelling to the dorsum of the hand and wrist without any real redness, and a linear abrasion that is dry and appears uninfected. On palpation, there is tenderness to the dorsum of the wrist and maybe slight warmth. On range of motion testing, there is limitation of both wrist extension and ability to extend the middle 3 fingers.

You are intrigued, so you show a colleague who tells you that it doesn’t look infected and he thinks the patient has a wrist drop that is unrelated, probably from how he slept last night. You do concede that Sunday morning is the best day to make a diagnosis of Saturday night palsy, but you go with your gut that something more sinister is going on. After all, there was a cat scratch, and the patient seems able to extend his thumb and pinky just fine.
You call your hand surgeon and ask him to come in and see if he wants to take the patient to the OR. What he says is so predictable, “What is the white count?” “It’s only 6.3,” you answer “But there is almost a left shift, 67% polys.” “Put him on Unasyn, have the hospitalist admit him, and I’ll see him tomorrow,” is his response. “I’m not comfortable with that because he already has significant disability,” you counter. “OK, I’ll come see him this afternoon in the hospital. Just get him admitted,” the hand surgeon concludes.
You are not sure this is the best treatment plan for your patient. You think he may need to go to the OR ASAP. Although the hand does not appear impressive, you are worried he has a purulent extensor tenosynovitis. You decide a picture may give your consultant the extra motivation he needs to do the right thing.


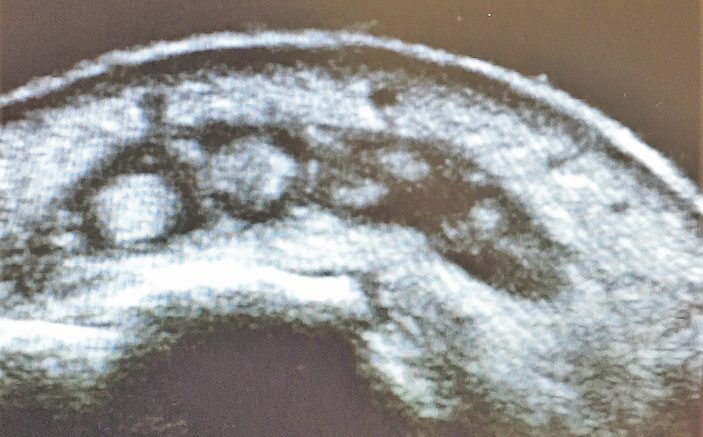
Ultrasound of the dorsum of the affected hand on the top along with comparison view of the normal hand below. These were both taken with water immersion.

Questions: What does the image show? What should you do next?
The labeled image below shows fluid surrounding thickened extensor tendons along with edema. The ultrasound was far more impressive than the physical exam in terms of swelling. The skin, tendons, bone, and edematous tissue on the image below all appear white/hyperechoic. The subcutaneous fat, blood within those juicy hand veins, pus and shadowing behind the dorsal cortex of the metacarpals all appear black/hypoechoic. A slightly more proximal view, also labeled below, shows more pus and less echoic tendons. At surgery, this was the area where the finger extensor tendons were noted to be slowly disintegrating leading to the patient’s inability to fully extend the fingers. He had a rocky course with multiple surgeries and still has residual disability.



Soft tissue ultrasound has many potential applications including evaluation for abscess, foreign bodies, joint effusion, tendon injury, to name a few. Another application is nerve localization for nerve blocks. In this case, point of care ultrasound (POCUS) was used to improve patient care by convincing a consultant to perform emergency surgery rather than wait until the following day, when tendon damage likely would have been even more severe.
Pearls and Pitfalls: Performing Tendon Ultrasound
- Probe and Positioning: Use a high frequency linear array transducer (10-13 MHz). Apply a large amount of ultrasound gel to improve your acoustic interface. For very superficial structures, use a stand-off pad, such as a bag of saline, or if practical, employ water immersion for even better images.
- Target Confirmation: Obtain images in multiple planes (longitudinal, transverse, oblique) and utilize the contra-lateral side for comparison when available.
- Bones: Bones have a hyperechoic outer service with hypoechoic posterior shadowing. Ultrasound can be used to identify fractures when a x-ray is delayed or unavailable.
- Muscle: Skeletal muscle will appear hypoechoic with interwoven echogenic striations and hyperechoic fascial planes. Muscle tears and intramuscular hematomas can be identified by ultrasound.
- Tendon Injury: Tendons appear brightly hyperechoic with visible linear fibers on long-axis scanning. Remember that normal function can be seen on physical exam with 90% tendon disruption. Partial or small tears can be assessed via bedside ultrasonography. Any hypoechoic or anechoic interruption in the hyperechoic tendon fibers should raise the suspicion of a tendon disruption. Subtle tendon damage may display an increase in the tendon cross-sectional area due to localized edema in the absence of actual tearing of the tendon fibers. Compare the area of interest to adjacent segments. If the ultrasound beam is not aimed directly parallel to the tendon fibers, a false hypoechogenicity artifact may be noted (anisotropy).
- Tenosyovitis: Fluid surrounding tendons will appear anechoic or hypoechoic and may signify infection or gout. It can also show tendonous attenuation from a destructive infection. If infection is suspected, immediate surgical drainage is usually indicated.
- Practice, Practice, Practice: The best way to minimize errors is through experience, so scan lots of normal anatomy. The more scans you do, the better you will be able to differentiate abnormal from normal, even when you may not be sure exactly what the abnormality is. An image library of normal and abnormal scans helps immensely, so dig back into the Soundings archive.
2 Comments
I thought the extensor tendons did not have fascia coverings like the flexor tendons did. I’ve been told there is “no such thing” as tenosynovitis of the extensors.
There is a distinction between fasciitis and tenosynovitis. According to UptoDate: “Extensor and flexor tendon sheaths have two surfaces: an inner visceral layer (visceral paratenon) adherent to the tendon and an outer parietal layer (parietal paratenon) abutting adjacent structures such as adjacent muscles and retinacular structures. Normally, the visceral and parietal layers abut one another. In the setting of tenosynovitis, the potential space between these two layers may fill with inflammatory or purulent fluid.”