In this age of budget cuts and health care reform it is becoming increasingly important for each medical specialty to prove its value, and back those assertions up with real data. It is not uncommon in these discussions for emergency medicine to come under attack as cost-cutting policies hone in on reducing ED visits for non-urgent care.
A series of recent studies on physician economics fail to recognize the impact of emergency department referrals on total hospital revenue
In this age of budget cuts and health care reform it is becoming increasingly important for each medical specialty to prove its value, and back those assertions up with real data. It is not uncommon in these discussions for emergency medicine to come under attack as cost-cutting policies hone in on reducing ED visits for non-urgent care. In this line of discussion, ED visits are often wantonly labeled as costly and avoidable. But what do the numbers say?
Three important studies were published in recent months which, when combined with an understanding of how EDs interact with hospital admissions, turn these suppositions on their ear.
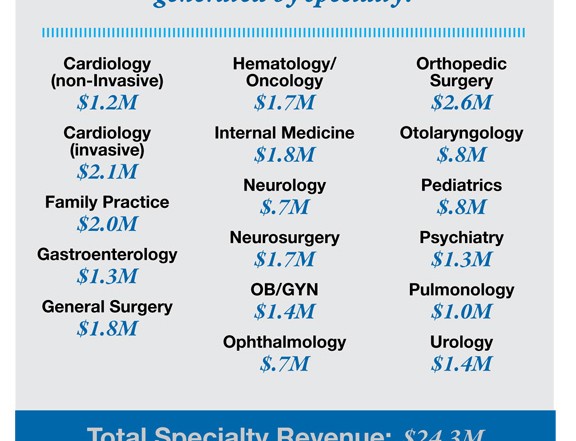
First is the Merritt Hawkins (MH) report “2013 Physician Inpatient/Outpatient Revenue Survey1”. This study assessed the annual inpatient/outpatient hospital revenue contributions of various specialties as a function of the average salaries of these physician groups. The key finding of this study shows orthopedic surgery at the top of the list with their revenue contribution being $2.6 M with an average salary of $519K. That comes out to a revenue-to-compensation ratio of 5.17:1. This calculation is made to make specialty comparisons more easily understood.
A complimentary article that appeared in Becker’s Hospital Review2 summarized the MH data and stratified it by specialty. Both sources stratify the specialties from orthopedic surgeons at $2.6 M to neurologists at $691K. The specialties rank order in terms of their revenue-to-compensation ration with family physicians at 10.94:1 at the top and otolaryngologists at the bottom at 2.00:1.
Those are some good, hard numbers upon which real financial decisions can be made, right? Not so fast. Conspicuously absent from the MH report is emergency medicine, suggesting perhaps the role of EPs in generating revenue is vastly misunderstood. Thankfully, our third study, The Rand Report, pulls the pieces together and helps us come to a striking conclusion.
The major relevant finding from the Rand Report is that “…Emergency physicians are increasingly serving as the major decision maker for approximately half of all hospital admissions in the United States.” Simply put, EPs have become responsible for 50% of inpatient admissions, and the decision to admit is a major revenue source for hospitals today.
What’s more, the Rand Report details that whether the emergency physician is admitting or not, they are providing increasingly complex examinations. “EDs support primary care practices by performing complex diagnostic workups and handling overflow, after-hours, and weekend demand for care.” Nearly all physicians questioned for the Rand study agreed that, “office-based physicians increasingly rely on EDs to evaluate complex patients with potentially serious problems, rather than managing these patient themselves.”
This finding is very consistent with Pitts3, who notes a rising acuity of ED patients as well as a more interventionist level of service being performed today in emergency departments. This ED patient complexity contributes first to hospital ED revenue, while the patients are in the ED and during their hospital stay, as well as the referrals of these patients both back to their PCPs, as well as to other specialists. This occurs both during the admissions as well as after discharge. ED physicians are contributing substantially to hospital revenue by being at the center of this multi-factorial series of care decisions.
So how can we assess the value of emergency medicine? What is the true revenue-to-compensation ratio that we should use?

In order to come up with a useful number, this article is going to suggest an estimated value for the percentage of revenue generated by other specialists that originated from emergency physician referrals. In an effort to not overshoot (while still recognizing the real contribution of emergency physicians) we will conservatively assume that emergency physicians contribute 15% of the inpatient and outpatient revenue generated by all other specialists. Coupling this assumption with the MH report and the fact that the average EP salary of $270,000, derived from the Medscape compensation report4, we get the following results:
- Of all specialist-generated revenue ($24.3M), 15% is attributable to emergency physician referrals ($3.6M)
$3.6M as a function of the average emergency physician salary ($270K) equates to a revenue-to-salary ratio of 13.5: 1 for emergency medicine - Conclusion #1: Using this assumption, emergency physicians would be the number one revenue generators for hospitals, among the noted specialties for both revenue and the revenue-to-salary ratio.
- Conclusion #2: Even if the referral percentage was lowered to 10 percent to be even more conservative, emergency medicine’s rank for revenue would be second at $2.4M and third for the revenue-to-salary ratio at 9.00:1.
This calculation substantiates and validates emergency medicine as a critical player in the emerging new world of healthcare. Emergency physicians are a major, if not the greatest revenue source for hospitals through admissions. Additionally, EM contributes to the entire downstream, outpatient revenue system through referrals after the patients’ ED visits conclude. Additional research will be needed to determine the exact percentage contribution of emergency medicine. However, the assumption above at minimum substantiates a starting point index of the value of emergency medicine in terms of real, recognizable numbers that cannot and should not be ignored. Emergency physicians are in many ways the nexus of care for the most critical patient populations – and revenue decisions – in today’s healthcare system. In the evolving world of increased scrutiny over service charges, it will become increasingly important to note these kinds of indices as measures of the value of emergency medicine regardless of the eventual outcome of the charge discussion. Hospitals survive on revenue and emergency physicians are a major contributor of that success.
John G. Holstein is a director of client development specializing in emergency medicine with Medical Management Professionals, Inc. (MMP).
References
- Merritt Hawkins. 2013 Physician Inpatient/Outpatient Revenue Survey.
- Herman, Bob. “51 Statistics on Physician Salaries vs. Hospital Revenue Generated.” Becker’s Hospital Review. May 14, 2013.
- Pitts, Stephen R. MD. “Higher Complexity ED Billing Codes-Sicker Patients, More Intensive Practice, or Improper Payments?” NEJM. Vol. 367. 12/27/2012.
- Medscape. Physician Compensation Report 2013.
1 Comment
Nice job, John. Some might argue with the assumptions and estimates, but it’s hard to negate the conclusions. For the skeptical hospital bean counter, or CEO: spend 8 hours (preferably on a Monday morning or a Friday evening) in the ED shadowing an ER doc, and all will become clear. Bring your running shoes.