
Laryngoscopy in infants and small children is a technically easier procedure than in adults. Mouth opening, jaw joint mobility, and dentition are all more favorable for laryngeal exposure in children vs adults.
Laryngoscopy in infants and small children is a technically easier procedure than in adults. Mouth opening, jaw joint mobility, and dentition are all more favorable for laryngeal exposure in children vs adults. Smaller diameter tracheal tubes relative to the lumen of laryngoscope blades make tube insertion and target visualization easier as well. For emergency care providers who rarely intubate children, however, the procedure can be intimidating. The principals of best practice laryngoscopy are even more important in infants and children; these include epiglottoscopy, progressive visualization of landmarks, and bimanual laryngoscopy.
The pediatric airway differs from adult airways in four main respects. First, the larynx is positioned higher in the neck. At birth the larynx is at the level of the third cervical vertebra. By adulthood it is at the level of the fifth vertebra. This explains why the epiglottis is often visible when examining the pharynx of a child, while it is rarely seen in adults. This difference makes it very easy to miss the main landmark of laryngoscopy, the epiglottis, with initial blade insertion. This error, the most common error of novice laryngoscopists, is exacerbated by operator nervousness.


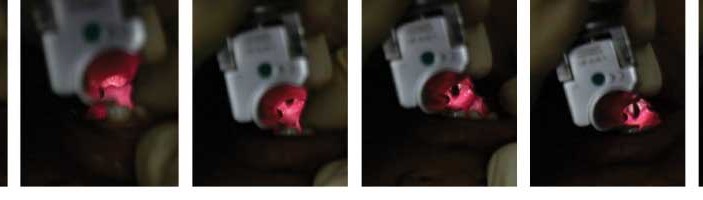
^The initial landmark on insertion into the mouth is the uvula (1), followed by the epiglottic edge (2). After tilting the blade posteriorly, the blade is advanced slightly, this time lifting the epiglottis, and exposing the posterior cartilages. Images 4 and 5 show the glottic opening and vocal cords. The endotracheal tube is seen between the vocal cords in image 6.

^Steps in pediatric laryngoscopy: Image 1 shows enlarged kissing tonsils and the next landmark seen is the epiglottis (2). The posterior cartilages comes in view and some of the glottic opening, after which is seen the true vocal cords (images 3 and 4). The upper lip retracted in image 5, just prior to tube insertion, using the extreme corner of the mouth (6).
When inserting the laryngoscope, a methodical, deliberately slow advancement of the blade will expose the epiglottis edge. During laryngoscopy in infants the epiglottis and uvula are often touching; the epiglottis may be located within an inch of the mouth. Often the epiglottis lies against the posterior pharynx, and it is critical to have a Yankauer to dab the posterior pharynx as the laryngoscope is advanced. Hyperextension of the head pushes the base of tongue and epiglottis backwards against the posterior pharyngeal wall, and makes epiglottis identification more difficult. The face plane of the patient should always be parallel to the ceiling (not tilted backward). Proper head positioning is defined as horizontal alignment of the ear and sternal notch. In small children a large occiput already elevates the head relative to the chest, so additional head elevation is not needed. In the smallest infants alignment of the ear and sternal notch may require slight support under the shoulders.
Any fluids, saliva, blood, or vomitus, accumulating in the posterior pharynx can camouflage the epiglottis, since the epiglottis often has the same mucosal appearance. Although tongue control is essential and critical for proper tube delivery, without deliberate identification of the epiglottis the procedure of laryngoscopy becomes a hit-or-miss experience of finding landmarks.
Chevalier Jackson, a pioneer of laryngoscopy and ENT surgery, considered identification of the epiglottis a prerequisite to exposure of the larynx. If necessary, I will sometimes advance the blade midline down the tongue, very slowly until the epiglottis is visible, and then I will move the blade over to obtain a right paraglossal location. Epiglottoscopy is a low-force aspect of the procedure. During epiglottoscopy, the mandible is being distracted inferiorly and slightly upward; only a slight grip on the laryngoscope is required (the thumb and 2nd and 3rd digits can lift the jaw). The mandible and tongue in small children weighs little. This phase of laryngoscopy is far less forceful than efforts at maximizing laryngeal exposure (the second part of the procedure), which includes much head lifting and force directed down the laryngoscope blade.
The mandible in infants and small children is under-developed, namely, it is shorter and narrower. This makes the displacement space smaller. A smaller displacement space favors use of a blade with a smaller displacement volume. Along with differences in epiglottis morphology, this is the reason for using a narrow lumen straight blade in small children instead of a large flange, large spatula, curved blade. Many providers familiar with curved blade laryngoscopy in adults do not appreciate the subtleties of straight blade laryngoscopy, especially when the landmarks are much smaller. The narrow flange of Miller blades should never be used to sweep the tongue to the left. The final position of a correctly placed Miller blade (in adults or children) is in a right paraglossal position. The base of the laryngoscope blade should be to the right of dental arch, aligned at or to the right of, the right nare of the patient. Not only does a right paraglossal placement assist with proper tongue control, but by staying to the right of the central dental arch, you will avoid impacting on the central dentition (and have more room). The smaller flange of straight blades can also make it more challenging for suctioning large volume fluids. In children between 4 and 8 years old who have large volume fluids in the oropharynx, I have sometimes found a Mac 2 blade easier for suctioning, since it provides easier tongue and jaw distraction and opens up a wider space. For patients age 4 and below, I almost always use a Miller or Wisconsin design (a slightly larger flanged straight blade).
The third difference in the pediatric airway is the increased size of the tongue relative to the size of the oral cavity. This redundancy of soft tissue in the upper airway requires very careful, progressive visualization of landmarks. Using a straight blade with a small flange can make epiglottis identification and effective tongue control challenging. Fortunately, the small diameter pediatric tracheal tubes, especially un-cuffed tubes, relative to the lumen of the laryngoscope blade, makes tube passage possible even when the tongue is not optimally controlled. In infants and small children a tracheal tube can fit through the appropriate Miller blade lumen, although it is never advantageous to block the line of sight (and not recommended).
A fourth difference in the pediatric airway is the relative increased length and stiffness of the epiglottis. The epiglottis is more difficult to control with indirect elevation. This is another reason to use a straight blade in small children. Not infrequently, it will be difficult after seeing the epiglottis to advance the blade just enough under the epiglottis (but not under the entire larynx). If its working, it is not illegal to use the Miller as a Mac, with the tip of the blade in the vallecula and indirectly elevate the epiglottis by pressure on the hyoepiglottic ligament.
Dr. Levitan teaches emergency medicine at Jefferson Medical College and at the Univ. of Maryland and helps run
a monthly airway management course involving specially prepared cadavers: jeffline.jefferson.edu/jeffcme/Airway