The average emergency physician will get sued at least once, if not several times in his or her career. The best defense against litigation, says Dr. Stephen Colucciello, is a “bullet proof” chart. The first step is to read the chief complaint and nurse’s notes to ensure that everyone is on the same page and that the chart is internally consistent. Then, anticipate the worst possible diagnosis and explain why you ruled it out. This can be done through statistics showing that your pre-test probability of a life threat based on history and physical alone is less than 1-3%. If the probability of a life threat is greater than this, then further testing will be needed. Also, pay great attention to vital signs and consider obtaining them upon discharge. If you’re particularly concerned about a patient then ask another doctor to see them or get a consultant on board. You can also get them close follow up such as a next-day appointment or even call them yourself the next day. Most importantly, act as if you were treating a family member.
2. When should I order a CT scan for my patient with pancreatitis?
The first indication for ordering a CT in a patient with pancreatitis, says Drs. Mel Herbert and Stuart Swadron, is if you’re unsure of the diagnosis. Lipase is a good test for pancreatitis but it is still not 100% sensitive. Therefore, in patients with a high index of suspicion for pancreatitis but with a low lipase level, CT will improve your diagnostic yield. If the diagnosis of pancreatitis has already been made, a CT should be considered in the ill-appearing patient. This can further guide management and act as a prognostic tool. Fluid collections around the pancreas are initially sterile but may become infected as evidenced by air within the peri-pancreatic fluid from gas forming organisms. At this point, the surgeon and interventional radiologist may become involved to culture the fluid and determine the need for surgery. More importantly, CT may show necrotic foci within the pancreas that will appear unperfused by the IV contrast. This will change ED management because broad spectrum antibiotics, which have been shown to decrease mortality, should be instituted immediately.
3. ALT elevation may be most predictive of a biliary origin of pancreatitis
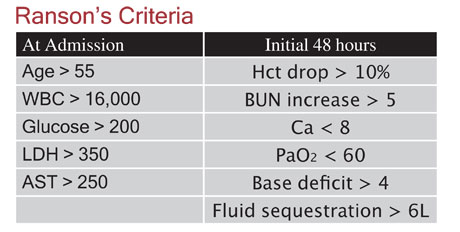
The priority in evaluating any patient with pancreatitis is to rule out surgically correctable causes of pancreatitis, namely gallstone pancreatitis. A review article from the Journal of Clinical Gastroenterology 1999, Volume 28(2) states that ALT may be “the most useful predictor of a biliary origin of pancreatitis”. In patients without a history of alcoholism, elevation of ALT two to three times above normal is 95% predictive of biliary origin of pancreatitis. Conversely, a normal ALT level does not rule out gallstone pancreatitis and further imaging should be obtained in most cases. An ED ultrasound may be appropriate for well-appearing patients with a low Ranson’s score, although a formal ultrasound should be ordered in patients that are ill-appearing. ERCP may be done in cases where the diagnosis remains uncertain, although this procedure may worsen pancreatitis.

4. “Airport malaria” may affect travelers to non-endemic areas
In a patient whom you highly suspect may have malaria, it might be necessary to obtain both the patient’s and the plane’s travel histories. “Airport malaria” are cases of malaria in and near international airports, among persons who have not recently traveled to areas where the disease is endemic. These represent cases of importation of infected Anopheles mosquito aboard an aircraft. This may be particularly dangerous because the physician has little reason to suspect malaria, particularly if there has been no recent travel to endemic areas. This delay in diagnosis may lead to a protracted course and death, especially in cases of Plasmodium falciparum. As a response, many aircrafts are “disinsected” if there has been recent travel to areas where vector borne diseases are endemic.
5. Indications for rabies prophylaxis
One of the new indications for rabies prophylaxis, says Dr. Billy Malone, is if a bat is found in the house. It is theorized that the virus may be aerosolized in the bat guano and subsequently inhaled. Therefore, it is recommended that everyone present in the house with the bat should receive vaccination. Interestingly, Dr. Malone states that “rabid dog” may be a misnomer because only 50% of dogs have the furious type of rabies, the other half being the paralytic type. Instead, “rabid cat” should probably be used because over 90% of cats have the furious type of rabies. What is reassuring is that there has been no dog-related rabies in the U.S. in over 30 years. However, beware of the limping dog in the third world. Any rabid animal bite in the third world is considered a trip-ender because of inadequate vaccine supplies in most third world countries.
1,033 patients across multiple institutions were studied to assess which factors led to noninvasive ventilation failure versus success (Eur Respir J 2005;25:348-55). A prediction chart using four criteria (pH, APACHE score, GCS, and respiratory rate) was constructed to assess failure rate. If all four of the criteria were abnormal on admission, the failure rate was 82%. Conversely, if all four criteria were reassuring, then patients had only a 6% chance of noninvasive ventilation failure. What was found to be more predictive was reassessment at 2 hours. If all four indices were negative at that time, then the failure rate was virtually 100% compared to 100% success rate if all four of the indices were reassuring. Therefore, a trial of noninvasive ventilation may be initiated on patients that are ill and may appear to require endotracheal intubation on initial assessment. If these patients do not significantly improve at the 2 hour checkpoint, then a definitive airway should be strongly considered.
For full summaries and audio downloads, as well as other CME opportunities, visit www.EMRAP.us.
18 Comments
A successful malpractice suit requires that the plaintiff prove a breach of the standard of care (liability) and that the breach was the proximate cause of injury (damage). In this case, there are questions about both elements.
The patient’s presenting complaint to the Emergency Department was tongue swelling. The patient had recently had erythromycin prescribed by his PCP. The patient reported that his PCP had heard a heart murmur and (presumably) the PCP had also noted a fever (or some other sign of infection) leading to the antibiotic prescription. The patient was febrile in the ED and reported that he had a murmur but the Emergency Physician did not hear it on auscultation.
The patient’s chief complaint was successfully addressed. The question of liability turns on an EP’s responsibility to pursue incidental findings, unrelated to the patient’s chief complaint. I think most EPs would agree that it is our responsibility to investigate incidental findings that may be an indication of serious illness. Fever and a new heart murmur should always raise suspicion of Bacterial Endocarditis. Bacterial Endocarditis is a serious illness. Therefore, in my opinion, the EP should have investigated further.
The diagnosis of Bacterial Endocarditis is proven by blood culture. The PCP was the first doctor to note the new murmur and (presumably) the fever. The PCP failed to send blood cultures and therefore is liable for failing to diagnose the pt’s condition. Since the EP did not hear any heart murmur, the prudent course might have been to send blood cultures and have the PCP follow up the result. In my opinion, the EP is liable for failing to do this. The PCP had a second chance when he saw the patient the next day and missed the boat again. It seems to me that the greater part of shared liability should be apportioned to the PCP.
As to damages, the patient remained undiagnosed for 4 weeks and suffered a stroke (presumably from a septic embolus) more than 2 weeks after initiating IV antibiotic therapy. Plaintiff’s expert testified that this bad outcome would have been avoided if the pt had been timely diagnosed by the EP. In my opinion, the expert is wrong. I know of no literature that correlates time to treatment of Bacterial Endocarditis with better or worse outcomes. Furthermore, embolic events in endocarditis can occur long after successful sterilization of the vegetation. Even common sense should lead one to see that failure to treat immediately is not a likely cause of an event that occurred after 4 weeks without treatment and more than 2 weeks of appropriate treatment.
So, in summary, it is my opinion that the EP bears a minority share of liability with the PCP for a breach of the standard of care. However, the failure to timely diagnose the pt’s Bacterial Endocarditis was not the proximate cause of the pt’s stroke and a jury should return a verdict of “no cause of action†in this case.
As is frequently the case in malpractice suits, an ounce of prevention could have averted a whole lot of grief for the doctor. Sending a blood culture, discussing the possibility of endocarditis with the PCP, and making a note in the chart that the PCP will follow up could have completely bullet-proofed the EP in this case.
comment one: everyone knows how hard it is to hear most heart murmurs in an overcrowded er, with wailing patients next door, separated by curtains? some murmurs are only appreciated on echocardiogram. Unlike most cardiologist, most of dont spend 5 minutes or longer listening for murmurs and then ordering echocardiograms regardless.
comment two: if the pcp was so concerned about bacterial endocarditis, he could have said so. The patietn could have been admitted. The EM physician was more concerned of the swollen tongue I figure, where a surgical airway was to be done. Not all pts with fever in the ed get blood cultures especially with runny nose, body aches, flu exposure, cough, headache, during flu season.
comment three: do the blood cultures x3 to get the greatest yield of an organism being caught but that doesnt mean the blood cultures won’t be negative.
In a case with fever w/o source, certainly one should try and get a good listen to the heart. If a murmur is heard, then the next question does it sound like a flow murmur due to fever, or something more “ugly.” If a strong mitral murmur is heard, an echo should be included ASAP.
We all see many patients with fever, and in flu season in particular it is very easy to overlook things. If the patient only had the fever on first visit a few days, I would bet many of us would miss it.
Did the patient even have endocarditis on the first visit? No way to know. But is going to be hard to defend when he TELLS you he has a murmur, you find no other source, and you don’t do blood cultures or document other risk factors for endocarditis, i.e. recent dental work, etc.
no substandard care is noted. there is no negligence and no causation. this is clearly a defense verdict. i do med/mal expert cases frequently and this is a winner for the defense.
Dr. Mitchell Heller is right on.
I agree with the statements that the EP should have paid attention to the “red flags” of fever and hx. of a heart murmur. As to the question of the preventability of the embulus by a timely diagnosis I do not know the answer; it’ll be settled by the ridiculous circus of malpractice court and “justice” will be rendered according to which clown (offense vs. defense) puts on a better show. Additionally, I think that we are missing part of this story : what diagnosis was made by the PCP who precribed the Erythromycin? Was this confirmed by the EP’s exam? Most of the time the EPs know a given PCP’s reputation. Are we dealing with a PCP who is regarded as competent? or is he the type who prescribes antibiotics as a kneejerk?
Final comment: swelling of the tongue, even transient is a potential for airway compromise; a period of observation in house may have been prudent.
First, a thanks to all who have commented so far, or who will join the dialogue. I just wanted to let everyone reading this know that we will be publishing the court verdict from the case that this scenario was based on in the April edition of Emergency Physicians Monthly, along with an analysis by Dr. William Sullivan, editor of the Standard of Care series.
I think we need to understand the question here. I think the variables are the patient/murmur/fever. The root question is whether the ED should be all things to all people.
I for one cannot meet the routine of care (“Standard of Care” is a misnomer in medicine: We mean the leader, the Standard Bearer. The Legal term refers the the average Joe Doc, the 50%-er, clearly not the best.) of each and every specialty and subspecialty in medicine.
I think we EP’s are testifying to the Routine of Care in a Routine (average) ED and need to be clear on this issue.
Thanks for the case.
Fortunately endocarditis is not a frequent occurrence in ER.However to reduce misdiagnosed cases more admissions and consultations are required. The critics wiill have a good day. I had a cardiologist against me in a malpractice case, who insisted that it was quite common, more often than not,for an acute myocardial infarction to cause a fever of 103.
The juries are selected,unreliable,often uneducated and have difficulties grasping the essential medical implications. In this endocarditis case, the education of the jury is vital important and the outcome will depend on the defense attorney and his ability to “show good bed-jury-manners”.(50 years ER)
Tremendous comments and a great forum here. Thanks for all the work that went into setting it up. I think that Dr. Benzoni has eloquently identified one of the great crisis of expectations that has developed in the malpractise world today. It is my observation over the last 20 years of medico-legal work that plaintiffs attorneys and experts are arguing successfully to juries that ED Docs should never miss anything. We are being held to a specialist and sub-specialist “best” standard of care and in fact are expected to be clairvoient as well.
Most ED’s are not even afforded the decent quality
stools, slit lamps, suture instruments, computer systems, etc. that are routinely found in ICU’s, CCU,s GI and Cath labs, OR’s SICU’s, etc. Dr. Torrez’s comments about the conditions under which we work are dead on. What amaze’s me is how much we do figure out under these conditions.
Last, but not least, does anybody believe that this patient had no further symptoms during the 4 week interval to diagnosis? Did the patient contribute by ignoring ongoing symptoms?
This case does not specify whether it was a new murmur or not. We see patients every day with murmurs and fever and do not automatically work up each for SBE. It is reasonable for the ED Doc to rely on the PMD to appropriately complete further work-up. I had a relatively recent case where i defended 2 ED Docs whose patient was subsequently seen 17 times over a 4 month period by Docs of 4 different specialties before a diagnosis was made. The plaintiff’s attorney argued for their culpability and the jury bought it assigning them $660,000 of the multi-million dollar verdict. That’s absurd. How can an ED expert testify to this in good conscience?
I look forward to hearing the outcome of this case.
Good case
I can’t tell from the case file whether or not the PMD put the patient on the emycin BECAUSE he knew the patient had a significant murmur and he had a fever and couldn’t find a source. If that were the case, then the need for blood cultures should have been discussed by the ERMD when he spoke to the private. I suspect that blood cultures would not have helped, but that is pure conjecture. Did the ERMD change the patients Abx to something else, and if so, what did he think he was treating, and if not what did he think the private was treating that no longer needed treatment, and did he do so with the private’s blessing. The fact that he saw his private again (at least once) and no further workup was ordered by him implies to me that the private did not hear any change in a longstanding murmur and felt further workup was unnecessary. If anyone is guilty of not meeting the standard of care here (and I am not sure anyone was) it would be the private MD. As to cause of the patients injury, I agree, there is no way you can blame the ERMD if this guy ran a fever for four weeks untreated and then had a stroke after two more weeks while being treated.
Classic, poor outcome so somebody must take the blame(and pay).
With murmur and fever, in a perfect world (like with academia-like resources and pace) the possibility of transesophageal echocardiogram with a set of blood cultures might have flashed on our radars and increased the probability of making a definititive diagnosis during the index ED visit. Of course those of us in the “blue collar” ER trenches this flash would be measured in nanoseconds. While there is no such thing as “bulletproof” documentation a note outlining an unambiguous(i.e. who, what, where and when) follow up plan might have been helpful.
The ED physician evaluated the patient, spoke to his PCP in real time, and the patient was seen in follow up by the PCP. The PCP had every opportunity to either alert the ED physician to the possibility of SBE by requesting (a) admitting the patient or (b) having blood cultures drawn and pursuing an outpatient echo. He chose not to. The ED physician met the standard of care; his failure to diagnose is not the proximate cause of the patient’s condition which manifested itself several weeks after the ED visit. To suggest that we should aggressively investigate incidental findings that aren’t acutely life-threatening is absurd. The patient had a mild anemia. I routinely don’t perform rectal exams on patients with a sore throat. Does this mean I’m liable for a GI bleed or cancer that’s diagnosed weeks later?
The above comments highlight how the tort process and plaintiff’s attorneys are using us to kill each other. Clearly there are those EM physicians who believe we should be all things to all people, and we are not allowed to miss anything – the “one and only chance” approach. It’s drummed into us in residency to avoid complacence, and it has it’s place in a training atmosphere. Unfortunately that does not transition well to the nonacademic setting where resources and consultants aren’t readily available. You try and do the best you can with what you’ve got.
Dr. Benzoni is dead-on. An expert who works in an academic or tertiary care center ED, with an availibity of resources unheard of in most community EDs, can’t with any degree of intellectual honesty testify as to the standard of care (what the average routine EM physician would do, given the circumstances) in a community hospital ED. I invite them to come work with me – full waiting room with no beds, 2 dozen boarders, no residents, no 24/7 ultrasound, limited or no specialists/subspecialists and oh by the way we don’t go on diversion. This is what’s it’s been like since before Christmas. Sound familiar to some people? It’s THOSE ED physicians that work in this environment who should determine if I met the standard of care.
Given the scenario, this pt. looked well and had no risk factors for endocarditis.He did not present with an infectious sounding chief complaint. If no murmur was heard, how could the poor sap who drew the short medicolegal straw by getting this guy poss entertain the dx of endocarditis? How many $millions$ are already wasted on neg blood c/s already? Does every pt without an infectious sounding cc and temp over 100 get blood cultures??
I read your spot on endocariditis and failure to diagnose. It poses the exact risk we take as ED docs everyday.
Never is the simple cold simple, nor the shoulder bursitis not an MI, nor the rash an underlying illness that cannot be diagnosed in one visit.
In particular, in this article, the physician can have an index of suspicion, however with a negative exam, no murmur, and no classic triad of symptoms as with certain disorders…….it is almost impossible to diagnose all conditions in one visit. That is why when patients are admitted or especially DISCHARGED, they need to follow up with a heath care provider. Also return to the ED if something changes or their symptoms get worse.
One can sue for failure to diagnose….however how can I diagnose the CVA that is impending when the patient comes for sutures and their BP is 160/98. How can I know that side pain after lifting is a kidney stone or early appendix, when the symptoms and onset support the evidence provided by the patients.
I love what I do, but the threat of a misdiagnosis for only 1 visit….. has force physicians to order tons of unnecessary tests and shoot for the moon in order to rule out EVERYTHING. I cannot practice that way. What was the point of medical school and experience, if you just use the shotgun approach.
This is clearly a tragedy for this patient. The PCP should definitely be asked to tell the court what his diagnosis was when he put the patient on Erythromycin for his fever. I have no doubt in my mind that this probably made the ER Physician skip the work up for the fever. He must have assumed that the PCP was already taking care of the pre-existing problem (the fever and the etiology).
I think there is a take home lesson from this tragic case. Never assume that the other doctor will get it straight.
I contracted subacute bacterial endocarditis in 2000. I did not know of any existing heart defects. I have now obtained all my notes and have discovered that A murmur was heard twice before I became ill. Once when I was admitted with a strep throat and the second time when I was attending an ante natal appointment. On neither of these occasions was the murmur followed up. They were simply resumed flow related murmurs. I then suffered from SBE for 1 year before it was diagnosed. By that stage it was too late and I needed a double valve replacement with a total of seven months in hospital. And so in response to Elise Zahn above….Patients are patients. They are not qualified to diagnose themselves. Otherwise why would they go to a doctor in the first place? When I presented at the doctor, I told him all of my symptoms. He diagnosed me with R Arthritis. I nearly died because he didn’t use a stethoscope once in a full year of illness. I now get a second opinion on everything. I’m lucky to be alive.