
Tips are useful in properly treating cyanotic congenital heart disease.
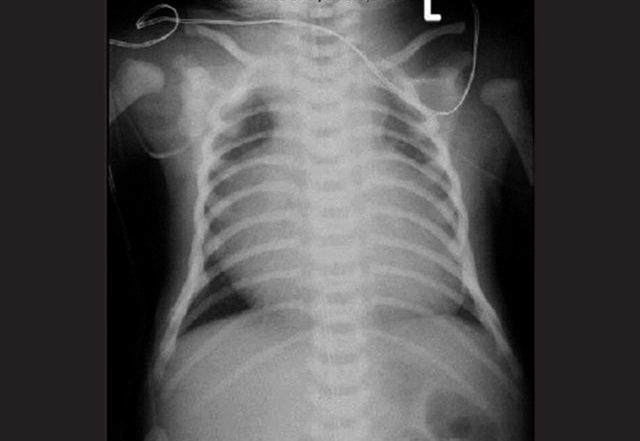
A 5-day-old female is brought to the emergency department with lethargy. Physical exam reveals an ill-appearing neonate with poor tone, cyanosis and delayed capillary refill. Point-of-care glucose is 55 mg/dL. Chest X-ray is shown below. What is the most appropriate next step in management?
A. Ceftriaxone

B. Dextrose
C. Epinephrine
D. Hydrocortisone
E. Prostaglandin E
Correct answer: E. Prostaglandin E
This neonate is in circulatory shock, the differential diagnosis of which includes sepsis, congenital heart disease and adrenal insufficiency. The chest X-ray shown demonstrates cardiomegaly, which combined with circulatory shock and cyanosis in the immediate neonatal period is most consistent with cyanotic congenital heart disease. Some congenital heart diseases are ductal-dependent, meaning that a patent ductus arteriosus (PDA) is required in order to be compatible with life.
As the ductus arteriosus closes naturally in the first few days of life, neonates with ductal-dependent congenital heart disease can develop circulatory shock. Transposition of the great vessels (TGV) is an example of a ductal-dependent congenital heart disease that also features cyanosis. Ductal-dependent congenital heart diseases that do not typically feature cyanosis include coarctation of the aorta, hypoplastic left heart syndrome, and aortic stenosis.
Treatment of circulatory shock due to suspected ductal-dependent congenital heart disease requires administration of prostaglandin E. Prostaglandin E preserves patency of the ductus arteriosus and can sustain peripheral perfusion until definitive surgical management can be performed.
The major ductal-dependent cyanotic lesions can be remembered by the “Five Terrible T’s”:
1-Truncus arteriosus
2-Transposition of the great arteries
3-Tricuspid atresia
4-Tetralogy of Fallot
5-Total anomalous pulmonary venous return
Incorrect answer choices:
Because sepsis is a common cause of circulatory shock in a neonate and can often be difficult to clinically differentiate from other causes of shock, empiric antibiotics are recommended for a patient with this presentation. Common regimens include ampicillin with gentamicin, or ampicillin with cefotaxime.
However, ceftriaxone (Choice A) in particular is a poor choice of antibiotic because it can cause biliary sludging, hyperbilirubinemia, and kernicterus in young neonates. Ill-appearing neonates are commonly hypoglycemic, in which case dextrose (Choice B) would be appropriate. The threshold for hypoglycemia in a neonate is a blood sugar level of about 35-45 mg/dL or lower, therefore the patient’s blood sugar of 55 is not responsible for her critical illness.
Epinephrine (Choice C) is a potent alpha and beta agonist that is used as adjunctive therapy in cardiac arrest in the neonatal period. It is not the primary treatment for suspected ductal-dependent congenital heart disease because its unpredictable effect on pulmonary and systemic vasoconstriction, preload and afterload has the potential to exacerbate the condition. Hydrocortisone (Choice D) is a corticosteroid used to treat adrenal insufficiency, which can be a cause of circulatory shock in the neonatal period. Neonates with severe adrenal insufficiency are typically hypoglycemic, which this patient is not.
References:
Yue EL, Meckler GD. Chapter 126: Congenital and Acquired Pediatric Heart Disease. In Tintinalli JE, Stapczynski JS, Ma OJ, Yealy DM, Meckler GD, Cline DM, eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide. 8th ed. New York, NY: McGraw-Hill; 2016.
Meckler G, Quereshi N, Al-Mogbil M, Kentab OY. Chapter 144: Metabolic Emergencies in Infants and Children. In Tintinalli JE, Stapczynski JS, Ma OJ, Yealy DM, Meckler GD, Cline DM, eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide. 8th ed. New York, NY: McGraw-Hill; 2016.
Collins SP, Storrow AB. Chapter 53: Acute Heart Failure. In Tintinalli JE, Stapczynski JS, Ma OJ, Yealy DM, Meckler GD, Cline DM, eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide. 8th ed. New York, NY: McGraw-Hill; 2016.