
Lack of medical staff in public emergency departments is in many ways a global phenomenon, so why should Hong Kong’s public emergency departments be singled out for special attention? Anyone who circuits the globe from country to conference and back will hear many similar stories of a critical shortage of emergency trainees and physicians.
Some EDs in Hong Kong have between a half and a quarter of the number of doctors per patient compared with other major metropolitian areas.
Lack of medical staff in public emergency departments is in many ways a global phenomenon, so why should Hong Kong’s public emergency departments be singled out for special attention? Anyone who circuits the globe from country to conference and back will hear many similar stories of a critical shortage of emergency trainees and physicians.

Hong Kong is not alone, and certainly does not have the worst healthcare statistics in the world. It boasts one of the longest average life expectancies for both males and females, despite spending about 5.2% GDP per annum on healthcare. So not all can be bad.
Hong Kong considers itself a ‘world class’ city and arguably has one of the six most developed emergency medicine specialties in the world. Along with the UK, USA, Canada, Australia and Singapore, it leads the world in the development of emergency medicine. The specialty in Hong Kong is now over 15 years old, and has its own College, Society, six-year training programme, 16 fully accredited emergency departments, over 450 specialists and trainees, a three-level examination system, and is sought after by overseas doctors for accreditation and training. So what’s the problem?
In the last five years, established physicians and new medical graduates have become increasingly disappointed, disinterested and disenchanted with the specialty. A decreasing number of new graduates are choosing emergency medicine as a career, and an increasing number of trainees and specialists are leaving for greener pastures. In recent years competition for vacant posts has decreased, and in some years up to 20% of training posts are unfilled.
Over the last 10 years hospital emergency care has come under increasing pressure. In some hospitals less than two thirds of emergency medicine posts have been filled, more than 60% training posts are vacant, and few, if any, new graduates apply for positions. Junior physicians rotate from other specialties for ‘service-training’ and general practitioner locums prop up the service. It is a tragic trend and a sad return to the past. Emergency trainees not uncommonly leave the specialty in their last year of training! Compare this with neighbouring Malaysia where nearly 400 graduates are on the waiting list for 34 national emergency medicine training posts. Food for thought.
Where have these emergency physicians gone and why did they leave? The real reasons may never be known but those departing leave the specialty for other careers, for the private sector (despite its poorly developed emergency system), to hospital management, and to general private practice. And why did they leave? The commonest reasons given are the unprotected and excessive workload, long patient waiting times, increasing numbers of critically ill and complicated patients who require complex assessment and management, insufficient resources, unreasonable work expectations, devalued staff, low morale, excessive night duties, overcrowding, severe access block, insufficient and unprotected training opportunities and poor promotion prospects. And there are no signs on the horizon that this situation will improve. Does this sound familiar?
More recently, waiting times for a first doctor-patient consultation in emergency departments have exceeded 24 hours, and the maximum number of patients waiting for that first medical consultation has reached 110. Some patients have waited over five days in emergency departments for a hospital bed, and some days up to 75 patients can wait longer than eight hours for a bed.
Access block is a major challenge in some emergency departments. In Hong Kong, access block is defined as any patient waiting longer than eight hours for admission to a hospital bed after the decision has been made that admission is required. Compare this with the recent National Health Service Report on Transforming Urgent and Emergency Care Services in England. ‘Recent data shows that the number of patients waiting more than four hours from the time of arrival at an A&E department to admission or discharge increased from 1.73 per cent to 4.1 per cent between 2009/10 and 2012/13.’ Hospital managers in Hong Kong balk at the thought of a true four-hour emergency department process time in Hong Kong. The average access block in some hospitals in Hong Kong was over 550 patients per month.
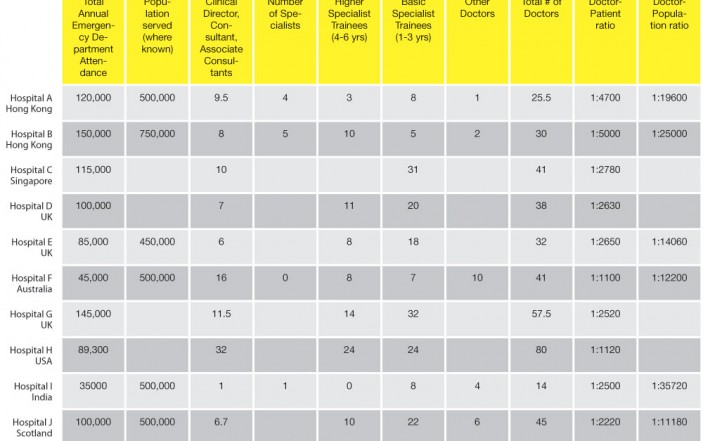
Table 1 shows a comparison between the medical staff to patient ratio from emergency departments in other international ‘world class’ settings with two leading departments in Hong Kong. This data was culled in 2007 but in the last five years there has been no improvement. Some emergency departments in Hong Kong have between a half and a quarter of the number of doctors per patient attendance compared with ratios of other world-class departments.
The reasons for this tragic situation are probably not unique to Hong Kong. For example, in some emergency departments in the UK, there is overcrowding, worsening admission block, an increasing complexity of cases being managed in the ED, deteriorating working conditions, lengthening waiting times, decreasing patient satisfaction, staff burn out and fewer new doctors joining and staying in the specialty. In 2012/13, in response to a patient satisfaction survey in the UK, it was considered shocking that ‘thirty-three per cent of respondents said they waited more than half an hour before they were first seen by a doctor or nurse – up from 24 per cent in 2004 and 29 per cent in 2008’! However, in Hong Kong, waiting times to first consultation may last as long as 24 hours.
The Way Ahead document jointly prepared in 2003 by the British Association for Emergency Medicine and the Faculty of Accident and Emergency Medicine (UK) provided recommended staffing levels for typical A&E Departments in the UK. For a department with an annual attendance of 100,000 patients, the recommendation was that there should be at least 36 doctors including eight consultants and 28 trainees, which would result in a doctor to patient attendance ratio of 1:2778.
Britain and Hong Kong have strong historical connections and similar health services and intended provisions of care. So how does Hong Kong compare with the UK? In a hospital in Hong Kong with an annual attendance of about 150,000 The Way Ahead suggests that about 54 doctors are needed to provide a reasonable service. In fact the number of allocated medical staff is 30 (15 specialist/consultants and 15 trainees), with a comparative shortfall of 55%. This assumes that all posts are filled.
Other specialties have well-defined roles, and emergency medicine is no different. The role of emergency medicine is to assess and to treat undifferentiated illness and injury. But unlike most other specialties, emergency medicine has a 24/7 open door policy, which leaves it open to ‘abuse’ from all quarters. Whilst other specialties largely retain their function, emergency medicine undergoes major role changes to meet the needs of society and the hospital. It is not only responsible for managing undifferentiated illness, and for hospital gate keeping, but also often acts as the buffer, pending zone and satellite for other specialties who cannot find a bed for a patient from their clinic.
In reality, the pressure on emergency care is a multi-faceted problem, which extends way beyond the emergency department, and apart from those mentioned there may be other reasons why the specialty in Hong Kong is in crisis. The underlying issues are partly historical and partly political. It started during the economic crises of 1997 and 2003 when high level decisions were made to reduce the numbers of students entering medical and nursing schools. This relieved the short-term pain of financial strain but set a course for even greater trouble. Next, the public, in general and understandably, do not want to increase taxes, do not want to pay for emergency care, and do not support a higher percentage of GDP allocated to healthcare. Yet there is an expectation that optimal care should be provided and also with minimal delay. This is not reasonable and not sustainable.
The result has been a squeeze on frontline emergency staff from the government and healthcare managers above, from the public below, and from other hospital and university departments alongside. When there is pressure from all sides eventually something must give, the bubble bursts, and the only perceived solution is to ‘get out’.
If things are so bad, then why isn’t anything being done about it? Again, there are many possible reasons. First, those in authority may fear to face the reality and enormity of the problem. The problem is perceived as too large to solve, too politically sensitive and so it may be better not to face it. Second, the shortage of doctors is not unique to emergency medicine but may also apply to many other specialties. Third, there may be a fear from academic sectors that the aging population with its poor prospects of any quality life whatever care they receive will flood the hospital system and affect medical student training, education, research and advancement. Hospitals in Wales have recently been in the headlines as increasing surgical waiting lists give way to a bitter winter of acute and unscheduled medical illness. Fourth, there are fears that an honest and transparent revelation of real and relevant data would discredit the authorities, the government and hospital managers. To voice this out would have an adverse effect on any individual’s hopes of development and promotion. Very few whistle blowers find an honoured place in history. Whilst there is little doubt that this situation adversely affects patient safety, taking the lid off the problem, and collecting and analyzing data, is thought to be too damaging politically.

So, what are the answers to these challenges? First, we need to acknowledge that this is a high priority, complex, multisystem problem that is most clearly evident in emergency medicine but actually involves all levels of healthcare and government. The whole hospital system needs to understand its responsibility – that this is a system, and not an emergency department problem, which needs rigorous assessment, root cause analysis and a multifactorial approach.
Second, politicians need to face these realities with honesty and transparency, adopting a long-term view for addressing the problem. This is not easy when political office is dependent on short-term appeal and votes. Politically it may be perceived as suicide to address these issues.
Third, are working conditions reasonable? Staff need to be valued and rewarded, and their lives and careers enhanced and protected. Job descriptions need to be attractive. Quality training needs to be provided and protected. It is not all about the patient. It is about the staff too.
Fourth, do tough decisions need to be made, and in some cases some services cut? It appears that there is a trend, despite insufficient resources, to increase rather than decrease services, and to build new hospitals and to expand specialties. Rather than produce high quality care for all, could this result in diluted, sub-standard and fragmented care for many? There is a need to contract and consolidate high quality care into fewer centres. Patients may have to travel further, but when they get to the hospital they will be assured of a high standard of specialist care, 24/7.
Fifth, the public need to be continually informed about its responsibility both in their use of services, and payment in taxes. A world-class service is expensive.
Sixth, do we need international benchmarking and risk adjusted mortality data on all aspects of care and between different models of provision? It is very convenient to say that Hong Kong’s situation is unique and that we should not compare apples and oranges. However, independent scrutiny and advice may bring much-needed direction.
Seven, we need more realistic and relevant methods of determining departmental staffing needs. Staff allocation is frequently determined based on number of patients registering annually in an emergency department. But with the changing and increasingly complex roles of emergency physicians, this is an outdated and simplistic concept which needs to be revisited. Should workload be redefined as the number of patient contacts rather than the number of patient attendances? For example, a patient waiting for admission for five days as a result of access block may need an additional five or more patient contacts, but at the moment they are simply counted as one registration.
Finally, do systems from other world-class settings need to be visited and learned from? Other cities less wealthy than Hong Kong provide better working conditions and emergency patient care than does Hong Kong. This needs to be acknowledged. What are these settings doing that we in Hong Kong are not doing? They have accountability, transparency, make tough decisions to benefit frontline staff and patients, and have a medium to long-term strategy that transcends the lifespan of a single government.
Hong Kong is not a poor city. Surely we can do better.
Professor Rainer has worked in Hong Kong for 17 years, and is currently Director of the Accident and Emergency Medicine Academic Unit at the Chinese University of Hong Kong and Honorary Consultant at the Emergency Medicine Department at the Prince of Wales Hospital, Hong Kong.
This article originally appeared in issue #11 of Emergency Physicians International. More at www.epijournal.com.