I want to save victims from cardiac arrest. I want to apply good CPR, use the right tools to improve outcomes, and use only the medications and processes that improve long-term restoration of neurologic function. Unfortunately, as Jimmy Buffett would say, “I arrived a little too late”.
Low cardiac arrest resuscitation rates are not only normal, they’re a sign of a healthy society and a successful emergency care system.
I want to save victims from cardiac arrest. I want to apply good CPR, use the right tools to improve outcomes, and use only the medications and processes that improve long-term restoration of neurologic function. Unfortunately, as Jimmy Buffett would say, “I arrived a little too late”.
And I’m not the only one. Across the country, emergency departments have seen a decline in resuscitation rates. What are we to make of this? Perhaps even more importantly, what are healthcare bean counters to make of this?
Before we start wringing our hands and investing millions in cardiac arrest training, let me say one thing: low resuscitation rates in the emergency department are not only OK, they are appropriate. In fact, they are actually a sign of the health of our citizens and a success story for the American emergency care system. We need to take a closer look at the numbers – and how they get skewed – so that we don’t divert healthcare funding away from preventative care, where it belongs.
Good News! Out-of-Hospital Cardiac Arrests on the Decline
For the years through the 1970s and 1980s, the American Heart Association utilized a statistic that about 675,000 Americans died of sudden cardiac arrest in the community. This number has sequentially decreased, and the burden of sudden cardiac arrest has decreased. The data is part of the CDC’s NHAMCS Emergency Department Data Summary Report. This survey has confirmed a marked decrease in the number of cardiac arrests, beginning with the initial survey conducted in 1992. In that year, it was estimated that 291,000 patients had CPR performed in American emergency departments. By the year 2002, the survey estimated that CPR was utilized on about 211,000 patients in EDs. The year 2008 continued the trend, with an incidence of patients where CPR was utilized of 119,000 patients.
Emergency department staffs have also found low rates of successful resuscitation, unless the patient arrests in the presence of the ED staff. This was confirmed in a study that noted a major decline in the incidence of out-of-hospital incidence of ventricular fibrillation, and in all cases of cardiac arrest presumably due to heart disease in Seattle. These are one set of data points that reflect the national decline of out-of-hospital cardiac arrest and coronary heart disease mortality(4).
Observation and longitudinal statistical studies indicate that cardiac arrest is a condition that should be prevented, and low resuscitation rates are the norm. In many communities, the most common presenting complaint of the cardiac arrest population is “My defibrillator fired!” These individuals walk out to the ambulance, or walk into the emergency department, and have had a cardiac arrest event. But the immediate consequence of the cardiac arrest is aborted by their implanted device, and almost uniformly those individuals have a good outcome. That is an effective health care system.
As Patient Populations Get Healthier, Cardiac Arrest Resuscitation Becomes More Like Trying to “Raise the Dead”
The results of attempted cardiac arrest resuscitation in sites other then airports and casinos is dismal, and in the study of that population, the rates of resuscitation will stay low no matter how much money is spend. The victims of cardiac arrest that are located in homes, nursing homes, businesses, and the streets are frequently not suffering from a disease process that is reversible. It is futile to assess an emergency system based on their inability to “raise the dead”. In areas where there are not effective end of life management programs, like hospice, there are frequent calls to EMS just because families don’t know how to manage an expected death and feel they need to call someone to “pronounce the person dead”. Unfortunately, many of those cases are managed, and included in the statistics, as cardiac arrests.
The result of these many processes is an apparent failure of cardiac resuscitation efforts by emergency personnel. This results in resources being misapplied to improve outcomes of cardiac arrest, rather then in primary prevention of premature death.

Case Studies: Ohio to Georgia
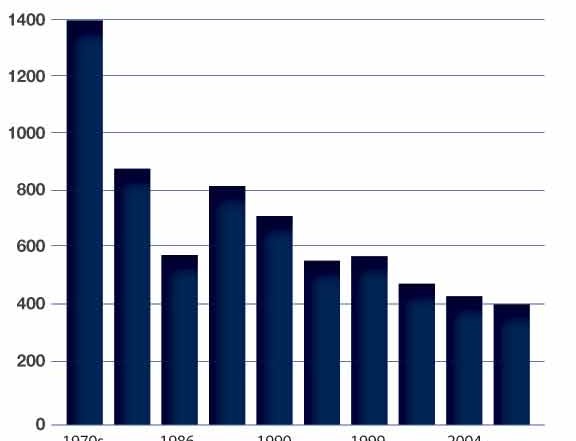
In longitudinal studies of cardiac arrest in the population of Dayton and Montgomery County, Ohio, there is additional evidence of changes in the cardiac arrest population. In that county, there has been a stable population for more then 30 years. The county’s fire department and EMS agencies were surveyed starting in 1980. In the early 1980s, those emergency providers treated about 1400 cardiac arrests a year, and pronounced an additional 700 patients a year at the scene. The number of cardiac arrest patients managed by EMS decreased dramatically in the late1980s. By the year 2000 the number of cardiac arrests per year stabilized at about 400 arrests, and about 700 times a year someone was found to be dead, and resuscitation was not attempted.
In reviewing the causes of death of the 400 cardiac arrest patients, the vast majority were found by EMS providers to be in a cardiac rhythm of asystole. This cardiac arrest rhythm is very unlikely to be associated with a short or long term successful resuscitation. That leaves a very small number of even potentially resuscitatable victims, under the best of circumstances. So the fire EMS services in the region can only report resuscitation rates under 10%, with many fewer then that surviving to a functional discharge from the hospital.
It could be interpreted that resuscitation rates in Montgomery County are low because care in the health system prevents the cardiac arrests that would be highly successful! This is a great success story! To improve cardiac arrest resuscitation rates it would be necessary to have more at-risk individuals suffer a cardiac arrest, and then resuscitate them from that condition. That would be done if the community’s health care providers would return to 1970s-style medical care, and let more 50 year old men go into cardiac arrest caused by sudden ventricular fibrillation. That would be counterproductive, and in that case, improved resuscitation numbers would be much to the detriment of community health.
In the study of cardiac arrests in Atlanta, Georgia over the last ten years, the numbers are almost the same. Atlanta Fire Rescue responds to about a cardiac arrest a day, serving a population of 500,000 citizens, and the airport. The resuscitation rates vary dramatically: There are very few successful resuscitations in the city, usually because the cardiac arrest victim has a large number of underlying medical problems, is older, and is found in asystole rhythm. At the same time, about 60% of the cardiac arrests at the airport are resuscitated.
Other Factors in the Success of Cardiac Arrest Resuscitation
The other element of community health that is strongly correlated with cardiac arrest rates and the success of resuscitation is the presence and effectiveness of hospice and other “end of life” programs. If the regional health system has excellent programs in those areas, people in the community are better educated about end-of-life occurrences, and for patients with terminal illnesses, EMS is not activated as frequently. Therefore, cardiac arrest population rate
s are lower, and success rates of those patients who have premature, unplanned and unexpected cardiac arrests can be higher.
Emergency department cardiac arrest outcome studies will also be influenced by EMS removal policies. In some cities, cardiac arrest victims that remain in asystole have CPR terminated in the field, and are not transported to the hospital. If EMS removes all cardiac arrest patients, the resuscitation rates in the ED will be very low. If EMS pronounces most patients in the field after failed resuscitation, then the ED rates can be higher. The community rates of cardiac arrest should be reported as part of a hospital’s resuscitation outcome data.
To understand the impact of cardiac arrest on a community, develop best practices, and apply community resources correctly, investigators should understand all aspects of cardiac arrest incidence. To investigate the rate of successful resuscitations that EMS and the Emergency Department participate in, EMS policy will have major impact In a comprehensive health care system.
For good reasons, and reasons that support good health practices, it is not surprising that there are low rates of resuscitation from cardiac arrest. Prevention of cardiac arrest is the key to a successful health system. Our highest risk patients often have their own defibrillators already in their chest! This is a success story for American health care, and we have missed the opportunity to celebrate!
References
1. McCaig, Linda F. National Hospital Ambulatory Medical Care Survey: 1992. Emergency Department Summary. Advanced Data. National Center for Health Statistics. US Department of Health and Human Services. No 245. March 2, 1994
2. McCaig, LF Ly N. National Hospital Ambulatory Medical Care Survey: 2000. Emergency Department Summary. . Advanced Data from vital and health statistics; National Center for Health Statistics. US Department of Health and Human Services. No 322. Hyattsville, MD. April 22, 2002
3. Niska RW, Bhulya, Farida, Xu, Jainmin. National Hospital Ambulatory Medical Care Survey: 2007. Emergency Department Summary. National Health Statistics reports number 26. US Department of Health and Human Services. Hyattsville, MD. August 6, 2010
4. Cobb LA, Fahrenbruch CE, Olsufka M, Copass MK. Changing incidence of out-of-hospital ventricular fibrillation, 1980–2000. JAMA. 2002; 288: 3008–3013
2 Comments
Dr. Augustine’s hypothesis is novel and worth considering: is the currently low survival rate from cardiac arrest in the United States a testament to our ability to prevent cardiac arrest in the first place? While I don’t pretend to know exactly all the reasons for our low resuscitation rate (and certainly an overly-inclusive resuscitation policy has something to do with it), there are some striking data inconsistent with Dr. Augustine’s hypothesis. For example, the actual average rate of survival is unchanged over the last 30 years (see Kellerman et al in Annals of Emergency Medicine), a timespan preceding the use of ICDs and many other significant healthcare advances. In addition, substantial variations in cardiac arrest survival exist between communities in the United States and abroad, suggesting either a co-localizing of important prearrest prognostic factors or, more likely, significant room for improvement in laggard communities. Consider that in Norway, which is listed 11th in the World Health Organization’s listing of most efficient healthcare systems, survival with favorable neurologic status doubled after implementation of post-arrest inpatient protocols to the current rate of 56% (yes that is not a typo). Meanwhile, the US has never reported anything close to that and is listed as #37 in the WHO rankings. Finally, a look at the Arizona experience will show that the survival rate in any one community is far from set in stone. Sure, there is an upper limit to survival from cardiac arrest. I just don’t think we can stop and say we’re at it. While I’m all for patting ourselves on the back, the data just don’t support well this hypothesis that we’ve put ourselves out of business by prevention and this line of reasoning may perversely lead to the potentially very real reason resuscitation rates are so low in this country: futilism.
I like this philosophy of less interventions in cardiac arrest. I have seen it many times, the cardiac arrest that goes on and on, and we don’t get a person back, only a brain death body with a beating heart. That is not fare for the patient, the family and society in general.