
How POC ultrasound can be of special benefit to ill or injured children
We know children are not simply little adults, but what are the specific differences when it comes to point of care Ultrasound?
Children have smaller body mass, more superficial internal organs, unique medical conditions and, of course, are less likely to cooperate with an undesirable or uncomfortable examination. With this in mind, let’s discuss the potential benefits of POC ultrasound for our junior patients.

Today, a 7-year-old girl was riding her bicycle on the sidewalk when struck by a vehicle backing out of a neighbor’s driveway. She was wearing an appropriately fitted helmet, but was noted to be pale, while complaining of shortness of breath, as well as left flank and thigh pain. EMS arrived quickly and immobilized her using a cervical collar and backboard. They were unable to obtain peripheral vascular access en route.
On arrival to the ED, she is awake and alert, but tachypneic and grunting. Abrasions and bruising are noted along her left chest. Your nurses report a blood pressure of 82/56 mmHg, oxygen saturation of 88%, and delayed capillary refill. Although her airway is clear, you are particularly concerned because you note diminished lung sounds over the left chest.
Here’s how you can use POC ultrasound to rapidly identify resuscitation priorities in our 7-year-old patient.

Figure 1. Lung ultrasound focusing on the pleura. In addition to normal pleural sliding noted during live scanning, the presence of comet tail artifact (arrow) in this patient provided strong reassurance against pneumothorax affecting the scanned lung segments.

Figure 2. B-lines are vertical densities extending from the pleura (arrow) throughout the entire depth of the scanning field. Three or more B-lines within one lung segment suggest increased interstitial lung water consistent with passive congestion, infection and/or inflammation involving that anatomic area.

Figure 3. Subcortical Color Doppler flow. The presence of color below (and not above) the bony cortex (arrow) following a small push of fluid through an inserted intraosseous line confirms appropriate sub-cortical placement.
You begin by placing a high frequency ultrasound probe on the anterior chest, looking for signs of a pneumothorax. Fortunately, your B-mode ultrasound demonstrates normal lung sliding and comet tail artifact in multiple sites over both hemithoraces. Satisified that your patient does not have a pneumothorax, you systematically scan through both lung fields and notice a number of hyperechoic B-lines extending throughout multiple lung segments on the left. In the setting of trauma, these lung rockets suggest an underlying left-sided pulmonary contusion. During your scan, your patient is placed on supplemental oxygen and her oxygen saturation levels rise to the low 90s.
After addressing her airway and breathing, you turn your attention to your patient’s hemodynamic status. Using a small phased array transducer, you obtain a parasternal long axis view of the heart and see a small and vigorously contracting heart without evidence of pericardial effusion. Assessing the right upper quadrant, you note hypoechoic fluid at the tip of the liver caudal to Morison’s pouch. You then assess the inferior vena cava and see that it collapses almost completely during inspiration. Although you worry that volume resuscitation may worsen respiratory difficulty resulting from the pulmonary contusion, you make the wise choice to restore volume first and call for an initial 20 cc/kg fluid bolus, as well as a type and crossmatch.
Nursing is unable to secure intravenous access, so you establish intraosseous access in the uninjured right proximal tibia. You immediately place a high frequency probe adjacent to the IO site while simultaneously providing a small initial fluid bolus and apply color Doppler over the site of interest. The presence of subcortical color in the absence of supracortical color confirms correct placement of the IO needle without extravasation. You can now proceed to administer the entire volume of IV fluids requested. Fluids initially improve her perfusion, but then respiratory distress worsens and her oxygen saturation decreases again. You decide to carefully intubate.
Following a successful intubation, your patient’s oxygen saturation initially improves, but within a few minutes, our child becomes mottled and her oxygen saturation decreases yet again. You observe rapid and vigorous bagging by the respiratory therapist. You reassess the pleura and continue to notice diffuse comet tail artifact but now observe a different quality of pleural movement. Instead of a rhythmic pulsatile motion of the pleura, you note a staccato movement. The lung pulse sign, in this situation, suggests hypoventilation due to mechanical hyperinflation. In addition to decreasing gas exchange, you are aware that increased positive intrathoracic pressure may compromise cardiac output. You direct the respiratory therapist to provide slower breaths at a considerably lower tidal volume. Lung sliding reappears while oxygenation and perfusion improve. You prepare for travel to the CT scanner.

Figure 4. Free fluid noted in the hepatorenal interface (Morison’s Pouch).

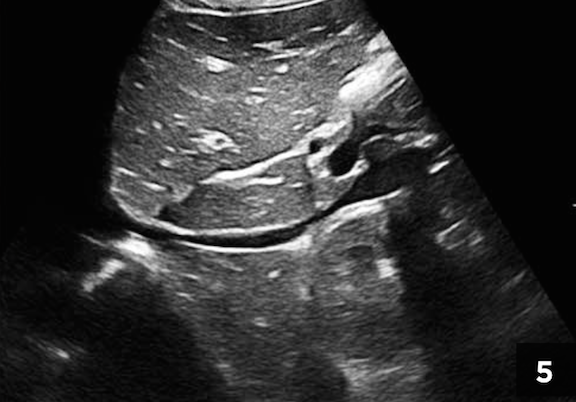
Figure 5. Long-axis view of the inferior vena cava taken at the onset of resuscitation. The generally small caliber and focal areas of almost complete collapsibility suggest hypovolemia.

Figure 6. Ultrasound-guided peripheral venous access. This long-axis view illustrates the catheter and needle (arrow) entering the target vessel.
CT confirms a pulmonary contusion, a Grade II spleen injury, and moderate hemoperitoneum. The pediatric trauma team arrives and a repeat FAST exam demonstrates no significant increase in free fluid within the abdomen. The surgeon agrees that the transient deterioration was more likely a result of the hemodynamic effects of the initial hyperinflation rather than continuing blood loss. Opting for observation as opposed to operative management, she requests peripheral intravenous access. With some patience and ultrasound guidance, you cannulate a peripheral vein in the right forearm and gratefully send this more stable and well-packaged child to the intensive care unit.
Important distinctions in pediatric point-of-care Ultrasound
- Children have a greater tendency to bend and not break. In our case scenario, the more cartilaginous and flexible pediatric thoracic cage absorbed and dissipated the force of impact throughout the involved hemithorax. The good news is a reduced tendency for rib fracture and complications such as pneumothorax while the bad news is greater prevalence of lung contusion. In addition, the pediatric liver and spleen protrude below the thoracic cage to a greater degree with their vulnerability compounded by generally less well-developed abdominal musculature.
- Traumatic hemoperitoneum in a child is not an absolute indication for laparotomy. Pediatric surgeons pioneered non-operative management strategies and successfully manage the vast majority of such cases conservatively, utilizing bed rest, serial hemoglobin measures and careful hemodynamic monitoring. Serial FAST examinations can complement other assessments.
- Pediatric blood pressures are often insensitive indicators of the presence of shock. Healthy vascular compartments allow for profound vasoconstriction and maintenance of blood pressure in the face of considerable volume depletion, potentially providing false reassurance of hemodynamic stability. Reacting only after the blood pressure drops is ill advised. The routine and repeated use of ultrasound for the assessment of volume status allows anticipation of fluid and transfusion needs in advance of later-appearing clinical manifestations of shock.
- Pediatric vascular access is often a difficult and stressful undertaking in the shocky pediatric patient. Although ultrasound-guided vascular access is extremely important, the technique is often time-consuming and may detract from initial efforts at patient stabilization. Conversely, ultrasound-verification of intraosseous needle position can occur virtually instantaneously using color-flow Doppler in synchrony with a small fluid push.
- Lung ultrasound may help guide fluid resuscitation. When caring for an ill or injured child, over-hydration may be as dangerous as under-hydration, suggesting the need for considerable precision. Ultrasound recognition of increased interstitial lung fluid has been utilized as a marker for third-spacing due to capillary leak resulting from infection, injury and/or over-zealous fluid administration. The potential of ultrasound for guidance of pediatric resuscitation–combining assessments of the heart, vascular capacitance and volume loss–is a potential game-changer.
1 Comment
With ultrasounds, it can be quite hard to tell what you are looking at if you don’t know what to look for. That is why it takes a trained professional to look at them. Given that there are many uses for this technology, it makes perfect sense to see that there are a lot of people using them.