You recently read a debate on the new American Heart Association guidelines for CPR on the blog WhiteCoat’s Call Room. Not long after, your local EMS director asks for your opinion about the evidence supporting compression-only CPR (COCPR) for witnessed cardiac arrest victims outside the hospital.
Should Cardiac Arrest First Responders Switch to Compression-Only CPR?
The Setup
You recently read a debate on the new American Heart Association guidelines for CPR on the blog WhiteCoat’s Call Room. Not long after, your local EMS director asks for your opinion about the evidence supporting compression-only CPR (COCPR) for witnessed cardiac arrest victims outside the hospital. While compression-only CPR would certainly be easier to teach bystanders, particularly for dispatchers real-time over the phone, you are uncomfortable following guidelines without some understanding of the research behind changing decades-old recommendations.
Your Options
- Accept AMA (and other) guideline dictates as gospel and move onto the next problem in your life without any personal research.
- Await the next national meeting of your preferred professional organization and hope that they will address this key question among their didactic offerings.
- Independently analyze the medical research surrounding these adjustments to long-standing CPR protocols and assess the strength of the evidence before implementing change locally.
The Critical Question
Does compression-only bystander CPR in witnessed arrest of presumed cardiac etiology improve patient-centric outcomes such as hospital survival or neurological recovery when compared with no CPR or conventional (ventilations + chest compressions) CPR?
Bottom Line
A statewide media campaign emphasizing COCPR increased bystander CPR rates. COCPR is independently associated with increased hospital-survival and good neurological recovery outcomes compared with conventional CPR or no CPR.
Background
In the United States about 300,000 individuals suffer an out-of-hospital cardiac arrest each year, but less than 30% have bystander CPR performed. Bystanders are usually not medically trained and a myriad of obstacles likely impede their willingness or ability to perform traditional ventilation-compression CPR including: reluctance to make mouth-to-mouth contact including fear of contracting infectious diseases, complexity of psychomotor requirements alternating between compressions and ventilations with incomplete understanding of anatomy and physiology, fear of causing harm, and panic. Data also suggests that interruptions in CPR can be detrimental. Therefore, any changes that remove or reduce some or all of these obstacles might reduce bystander’s time-to-CPR and CPR effectiveness. Given that bystanders most often are the first to attend to cardiac arrest patients, these changes could theoretically improve survival rates currently reported around 10% .
Theoretically, COCPR may have distinct advantages over conventional CPR by reducing the rapid deterioration of forward blood flow that occurs during chest compression disruptions and the significant time required to perform breaths. Animal models have previously demonstrated that COCPR is at least as effective as conventional CPR. In addition, three randomized controlled trials have already demonstrated that dispatcher-assisted CPR instructions comparing conventional CPR with COCPR favor the latter. Specifically, Hallstrom et al. noted a trend towards survival to hospital discharge with COCPR (COCPR 14.6% vs. CPR 10.4%, p=0.18), while Rea et al. (15.5% vs. 12.3%, p =0.09) and Svensson et al. (19.1% vs. 14.8%, p=0.16) noted similar non-statistically significant trends. Since each of these trials assessed dispatcher-assisted CPR, bystanders did not immediately initiate resuscitation.
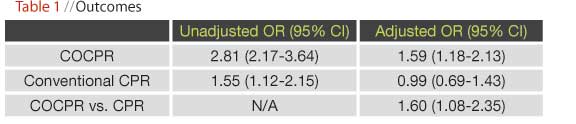
In 2005, healthcare leaders in Arizona recognized extremely poor outcomes for out-of-hospital cardiac arrest victims. Consequently, they implemented changes at multiple levels including EMS protocols to minimize interruptions in chest compressions during CPR as well as a statewide media campaign educating bystanders to use COCPR rather than conventional CPR (Table 1). In addition, they formed the Save Hearts in Arizona Registry and Education (SHARE) program that consisted of 30 EMS agencies in 2005 and grew to 90 agencies (serving 80% of the state’s population) by 2009. Arizona did not have dispatcher-assisted CPR programs during this interval.
The current research is a prospective, observational cohort analysis of the SHARE programs including all adult cardiac arrest victims between Jan 2005 and Dec 2009. All arrests were presumed to be cardiac arrests unless the events were known to be caused by trauma, drowning, asphyxia, or drug overdose. In-hospital cardiac arrests, resuscitations performed by bystanders with formal medical training, patients with obvious signs of death or with do-not-resuscitate orders were also excluded. EMS personnel collected all data prospectively into an Utstein-style database after receiving training on how to code bystander CPR (no CPR, conventional CPR, or COCPR). The primary outcomes were survival to hospital discharge and Cerebral Performance Category neurological outcome at hospital discharge. Multivariable logistic regression analysis was used to assess whether type of bystander CPR performed was independently associated with outcomes when adjusted for such confounding variables as age, gender, location, EMS dispatch time, initial rhythm, and therapeutic hypothermia.
Results
A total of 4493 patients were included in this analysis. The annual rate of bystander CPR increased significantly from 2005 to 2009 from 28.2% to 39.9%, corresponding with an increase in COCPR from 19.6% to 75.9%. During this time overall survival also increased from 3.7% to 9.8%. Logistic regression analysis demonstrated that COCPR was associated with an improved odds of survival compared with either no CPR or conventional CPR (see Table 2 where Odds Ratio > 1 indicates increased odds of surviving with that intervention). For cardiac arrest victims with a shockable rhythm upon EMS arrival, survival was 17.6% in no CPR, 17.7% in conventional CPR, and 33.7% in the COCPR groups. The investigators also recognized potential concerns about the unintended and untested use of COCPR in children under age 12-years where respiratory arrests predominate, but their analysis demonstrated that only 10/127 children (7.9%) received COCPR during this interval and that all types of bystander CPR had low overall survival rates in pediatric populations.

 Caveats
Caveats
This is an observational study subject to multiple biases that randomized controlled trials reduce via allocation of unrecognized/unmeasured confounding variables across treatment groups. It is an unfortunate (but real-world) limitation that the current trial could not be randomized since the intervention decision rests with the bystander at an unpredictable point in time when they are present to witness a cardiac arrest. The unmeasured confounding variables such as underlying comorbid disease burden, local bystander CPR competence, or EMS resuscitation proficiency could bias these findings and cannot be completely eradicated with statistical adjustments. However, the current trial is probably the best design that emergency providers can hope for with this clinical question.
One limitation that the investigators fail to address is the potential impact of a Hawthorne effect. While some experts debate whether this bias even exists, theoretically subjects or research assistants who are knowingly under investigation as part of a research protocol may adjust their actions in a way that they would not outside the research milieu. For example, bystanders who were aware that Arizona was leading the nation in incorporating minimally interrupted cardiac resuscitation might have been more likely to respond to a witnessed arrest or worked harder to perform skillful COCPR than would others who have not been exposed to a media blitz. In addition, EMS providers responsible for determining whether bystanders performed COCPR who are collecting data for SHARE might also be more aggressive about collecting data (ascertainment bias) or alter their ALS-protocols or institution of therapeutic hypothermia knowing that the results of their actions are being observed and systematically analyzed.
Finally, the investigators report logistic regression results in Odds Ratios (OR). These can be difficult for clinicians and patients to interpret. Using readily available online calculators (http://ktclearinghouse.ca/cebm/practise/ca/calculators/ortonnt), astute physician consumers of the healthcare literature can translate OR into Number Needed to Treat provided they have an estimate of the expected effect size. In the present example, the overall survival was 7.1% over the 5-years of the study and the adjusted OR for COCPR was 1.59 which translates into a NNT of 27. In other words, bystanders would have to perform COCPR on 27 cardiac arrest victims for one to survive who would not otherwise have survived.
The Outcome
After reviewing the SHARE data in conjunction with the weight of the evidence from Rea, Svenson, and others, you decide that the time has come for COCPR training in your layperson resuscitation courses. You advise your EMS director accordingly and provide him with links to the Arizona resources to begin modifying local educational initiatives.
6 Comments
Regarding the EBM case of the month, we noticed you have not yet posted the articles for December on the website, and it is now January?
Thank you for following this column so closely! While it’s an important part of our editorial line-up, we do not run an EBM article every single month. You are correct that we did not run one in December. Thank you for your interest!
What is the best foundational textbook for studying evidence based medicine?
EBM Reader:
My opinion:
1. Gordon Guyatt, et al. Users Guide to the Medical Literature: A Manual for Evidence-Based Clinical Practice, 2nd Edition, McGraw Hill (2008).
2. Weingart S, Wyer P; Emergency Medicine Decision Making: Critical Choices in Chaotic Environments, McGraw Hill (2006).
3. Straus SE, et al. Evidence Based Medicine: How to Practice and Teach EBM, 3rd Edition, Elsevier (2005)
4. Mayer D. Essential Evidence Based Medicine, 2nd Edition, Cambridge (2010).
The last two focus on diagnostics.
5. Newman TB, Kohn MA; Evidence-based diagnosis, Cambridge (2009).
6. Pines JM, Everett WW; Evidence-based emergency care: diagnostic testing and clinical decision rules, Blackwell (2008).
Chris Carpenter, MD, MSc
EPM Chief Clinical Editor
Thank you for the reading list. What is the threshold or “tipping point” for when a study changes practice?
Great question about the “tipping point”! A couple of resources to answer your question.
1) https://epmonthly.wpengine.com/features/current-features/secrets-to-healthy-skepticism/
2) Cone DC, Lewis RJ; Should this study change my practice? Acad Emerg Med 2003; 10: 417-422.