



Traumatic cardiac injuries are uncommon in the pediatric population. Of reported traumatic cardiac injuries, contusions account for 95% of injuries, and penetrating trauma is rare. We report the case of a 9-year-old girl who sustained a BB gun-associated penetrating cardiac injury that was complicated by a central nervous system stroke resulting from the BB pellet travelling intravascularly and lodging in the right common carotid artery. The BB path was deciphered using ultrasound. Because of the right common carotid artery obstruction, significant neurological deficits developed shortly after the injury. In addition to the case presentation, we present a review of the literature on penetrating cardiac injuries, missile emboli, and traumatic stroke in the pediatric population.
A previously healthy 9-year-old girl was accidentally shot at close range when she ran into the muzzle of a multi-pump cocked BB gun. She first presented to a local Emergency Department. The projectile entrance wound was in the left upper chest medial to the left axillary fold. She was initially asymptomatic and discharged home with no imaging.
After presenting to the local ED two additional times and her own pediatrician once for symptoms of ongoing weakness and seizure, she was transferred to the nearest tertiary care children’s hospital for further evaluation and consultation with a pediatric neurologist despite having a reportedly negative head CT.

ED VISIT #3
Upon presentation to the pediatric emergency department, the patient demonstrated obvious and severe neurologic deficits. An MRI head was attempted but was aborted due to the discovery of an artifact suggestive of metal. Skull films were then performed, and these studies demonstrated a round foreign body in the cranium approximately the size of a BB. The location, posterior to the right orbit, corresponded approximately to the right common carotid artery. After consultation with the neurosurgical attending, immediate interventions were deferred, but an angiographic study was recommended and scheduled for the next morning. She was transferred to the pediatric intensive care unit.
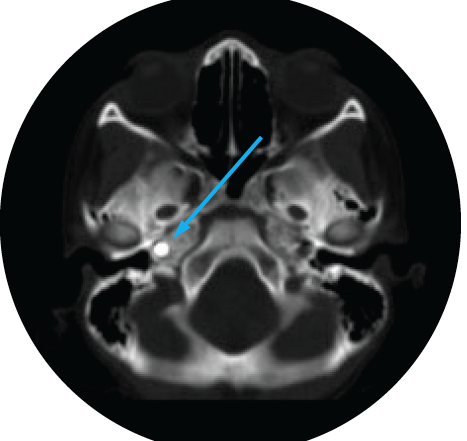
A CT head with and without contrast was performed. Complete thrombosis of the cervical right internal carotid artery distal to the internal carotid artery/external carotid bifurcation was noted with thrombosis extending to the cavernous segment. The thrombosis was attributed to the presence of a foreign body within the petrous canal (See figure 1).
Fig 1. CT image of head shows a transverse image without contrast-showing round metallic object posterior to right orbit:


THE MOVING BULLET
Initially, it was unclear how the BB had migrated to the right internal carotid artery distal to the internal arotid/external carotid bifurcation when the initial BB wound was in the left chest medial to the left axillary fold. Subsequent findings, however, provided an explanation. A troponin I was found to be critically elevated at 1.939 ng/ml. An echocardiogram demonstrated a structurally normal heart, but a small echogenic linear density consistent with a BB tract was noted in the left lateral ventricular wall at the base of the papillary muscle. No wall motion abnormalities were noted, and there was no evidence of an intracardiac shunt by saline contrast injection. The left ventricular shortening fraction was within the normal range.
There was also no evidence of a pericardial effusion or ventricular wall aneurysm. These findings were considered evidence that the BB had gone through the left ventricle. (See figure 2 and 3) After the BB had entered the arterial circulation from the lateral left ventricle, it embolized to the right side. The patient had medical management with anticoagulation after surgical management was felt to be a higher risk than benefit.
Fig 2. Echo image, apical two chamber view of left ventricle showing projectile tract through left ventricular lateral wall demonstrated by blue arrow:


Fig 3. Echo image, parasternal short axis view of left ventricle showing projectile tract through left ventricular lateral wall demonstrated by blue arrow:

After extensive rehabilitation, the patient has made a significant recovery. She is followed by neurology, and her ongoing medication are levetiracetam 300 mg bid (20mg/kg), aspirin 81 mg daily, and Prozac 10 mg daily.
DISCUSSION
This is a unique case where the application of ultrasound provided critical information to explain the path of the embolized BB pellet, from the lateral left ventricle to the right internal carotid artery causing stroke. Although the BB pellet was not visualized, the tract that it left behind did prove to be essential in deciphering the bullets’ migration. To our knowledge, this is the only documented case of a pediatric patient with penetration of the left ventricle by a BB pellet that migrated to the right internal carotid artery causing a stroke. There are very few cases reported in the adult literature. [4,9,10]
Generally speaking, when dealing with a penetrating missile injury without a corresponding exit wound, arterial embolism should be a consideration. Similarly, if there is radiologic evidence of a projectile in an unusual anatomic site that has no anatomic relationship to the observed entrance wound, one should consider embolization. [13-14,16,18-20]

When an intravascular bullet migration is suspected, it must be localized in order to determine the best approach for its removal. Treatment modalities used in the past have included anticoagulation, surgical intervention, and supportive care. Because of the rarity of traumatic ICA thrombosis, it is unclear which treatment is the most appropriate. General supportive measures and prompt involvement of the appropriate specialists is the emergency department mainstay for management of the pediatric stroke patient.
CONCLUSION
Air guns can be dangerous and have the potential to cause severe injury. Because of their relatively low velocity and favorable shape, BBs and pellets are prone to embolization, and this diagnosis should be considered when no exit point is found after penetrating injuries—even more specifically when the heart may have been penetrated. Elevated troponin and cardiac ultrasound may help reveal suspected injury and trajectory, although further investigation is warranted. A thorough radiographic survey should be performed if the foreign object cannot be located. [8]
REFERENCES
1. Bertoldo U, Enrichens F, Comba A, et al. Retrograde venous bullet embolism: a rare occurrence case report and literature review. J Trauma. 2004;57:187-192.
2. Morales JM, Patel SG, Monarrez C, et al. Air pellet embolization after penetrating cardiac injury. J Trauma. 2000;49:774-775
3. Wallace KL, Slovis CM. Hepatic vein bullet embolus as a complication of left thoracic gunshot injury. Ann Emerg Med. 1987;18:102-104
4. Dadsetan MR, Jinkins JR. Peripheral vascular gunshot bul let embolus migration to the cerebral circulation. Neuroradiology. 1990;32:516-519
5. Schmelzer V, Mendez-Picon G, Gervin AS. Case report: trans thoracic retrograde venous bullet embolization. J Trauma. 1989;29:525-527.
6. Shannon FL, McCroskey BL, Moore EE. Venous bullet embolism: rationale for mandatory extraction. J Trauma. 1987;27:1118-1122.
7. Van Way CW III. Intrathoracic and intravascular migratory foreign bodies. Surg Clin North Am. 1989;69:125-133.
8. Michelassi F, Pietrabissa A, Ferrari M. Bullet emboli to the systemic and venous circulation. Surgery. 1990;107:239-245.
9. Colquhoun IW, Jamieson MP, Pollock JCS. Venous bullet embolism: a complication of airgun pellet injuries. Scott Med J. 1991;36:16-17
10. Alsofrom DJ, Marcus NH, Seigel RS, et al. Shotgun pellet embolization from the chest to the middle cerebral arteries. J Trauma. 1982;22:155