
ECG findings you don’t want to miss.
A 56-year-old male presents to your emergency department complaining of substernal chest pain, mild dyspnea and fatigue. He has a history of hyperlipidemia and hypertension. You obtain an electrocardiogram, but are not sure whether it represents acute MI as it does not meet traditional STEMI criteria.
Background
The classical STEMI criteria were developed to ensure that obvious myocardial infarction is not missed in the acute setting.[1] However, emergency providers must be familiar with many other ECG manifestations of acute coronary artery occlusion. “STEMI” is only one of many potential presentations of Occlusion Myocardial Infarction (OMI), as described by Drs. Pendell Meyers, Scott Weingart and Stephen Smith.[2] This article will cover a number of commonly missed ECG findings indicative of OMI and require urgent cardiac catheterization.

There are a few principles that apply to diagnosis of OMI in every case. The first is that serial ECGs should be performed in all cases where acute coronary syndrome is suspected. This can prevent missing an obvious OMI as ECG findings can evolve over a very short (often 5-15 minutes) period of time.
Changes in ST segment or T-wave morphology over a short period of time are strongly suggestive of an unstable coronary lesion requiring intervention.[3] Absence of changes does not mean the patient no longer requires emergent catheterization. The effects of nitroglycerin on ECG findings are unclear, but obtaining an ECG prior to administration allows providers to trend potential changes. It is also important to evaluate any prehospital ECGs that have been recorded. It is possible that changes have resolved prior to the emergency department ECG due to prehospital treatment or spontaneous improvement. Computer ECG interpretation will frequently miss subtle or atypical findings, and may interpret the ECG as normal. The interpreting clinician must ensure details are not overlooked.
Subtle Inferior OMI
Inferior myocardial infarction frequently presents with few early ECG findings so it is important to be able to recognize subtle signs. Inferior OMI presents with ST-elevation in a combination of leads II, III and aVF. However, the earliest finding is often T-wave inversion or ST-depression in lead aVL.[4,5] This is a reciprocal change, but can present prior to ST-elevation. Additionally, in the inferior leads, the first changes may be an increase in T-wave width and height.


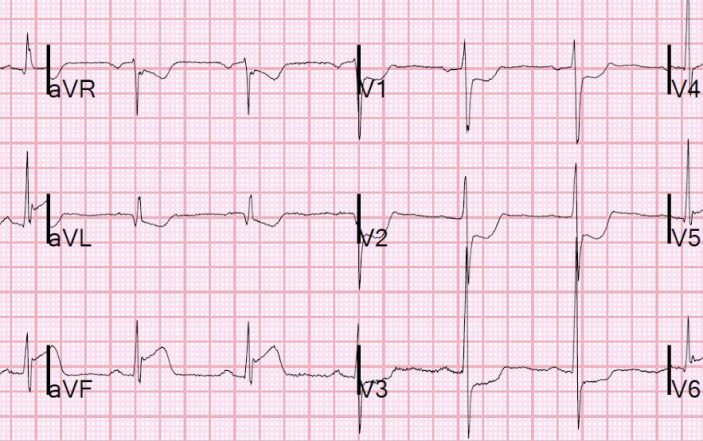
De Winter’s T-Waves
A lesser known presentation of acute occlusion or near-occlusion of the left anterior descending (LAD) is de Winter’s T-waves, first published by de Winter in 2008.[6] The condition is characterized by ST depression and hyperacute T-waves in the distribution of ischemia. These are not reciprocal findings, or indicative of posterior infarction. Importantly, these patients may have had resolution of symptoms, since de Winter’s T-waves can indicate near or intermittent occlusion.

OMI in Left Bundle Branch Block or Right Ventricular Pacemaker
It is classically believed that the ECG cannot be used to diagnose acute OMI in the setting of left bundle branch block (LBBB) or in patients with a right ventricular pacemaker, which generates a LBBB pattern. It has historically been taught that patients with new- or presumed-new LBBB, should be treated as if they are having a STEMI if they present with ACS symptoms. Both of these ideas are flawed as the modified Sgarbossa criteria can be used in both scenarios to diagnose transmural ischemia.[7–9]
The idea is to recognize ST elevation, which is excessively discordant (in the opposite direction) with the QRS complex or any ST elevation that is concordant (in the same direction) with the QRS complex. The criteria for the modified Sgarbossa criteria are:
- At least 1 mm of concordant ST elevation in at least one lead*
- At least 1 mm of concordant ST depression in at least one of leads V1-V3*
- At least 1 mm of discordant ST elevation and an ST elevation to S-wave ratio of at least 25% in at least one lead.
*any amount of concordant change is likely abnormal may indicate OMI


Posterior Myocardial Infarction
The typical ECG findings of posterior OMI are ST depression in any of the leads V1-V4.[10] Those leads are essentially seeing a mirror image of the posterior wall causing ST depression instead of ST elevation. Also, note that ST depression in these leads is NOT anterior wall ischemia or a reciprocal change, but posterior infarction, which is commonly misunderstood.[11]
Performing a posterior ECG with leads V7-V9 is less sensitive and specific than the findings seen in V1-V4, but posterior leads may be useful in some cases.[10] Posterior infarct is associated with lack of flow through the posterior descending artery (PDA) which may be supplied by either the right coronary artery (RCA) or left circumflex artery (LCx). It is common to see posterior infarct in association with inferior or lateral OMI, but can also be seen in isolation due to occlusion of the PDA or distal occlusion of the RCA or LCx. Contrary to widespread belief, the T-wave may be inverted or upright, dependent on the balance between anterior vs. posterior wall T-wave forces, the duration of occlusion and the state of any spontaneous reperfusion. In addition, ST depression of posterior MI generally has maximal ST depression in V2-V4, whereas the ST depression of subendocardial ischemia is more often in V4-V6. On occasion, ST depression maximal in V2-V4 is due to subendocardial ischemia.

Subtle LAD Occlusion
Differentiating between anterior OMI and benign early repolarization is challenging. ST elevation is a normal finding in some patients. One key to diagnosis in these patients is serial ECGs, which can show dynamic changes indicating OMI. Additionally, comparing to a patient’s prior ECG, when available, can aid in diagnosis.
A calculator was developed by Dr. Smith to distinguish between LAD occlusion and benign early repolarization.12 This is available on MDCalc, Dr. Smith’s ECG Blog, or as a standalone app on Apple iOS titled “SubtleSTEMI” and on Android titled “ECG SMITH.” It requires four measurements:
1) ST Elevation at 60 ms after the J-point in lead V3 (STE60V3)
2) computerized QTc
3) R-wave amplitude in V4 (RAV4)
4) total QRS amplitude in V2 (QRSV2).
A result greater than 18.2 has been validated as supporting LAD occlusion over early repolarization.



Pericarditis or OMI?
Pericarditis is one of the most common mimics of OMI. Traditionally, it is taught that diffuse ST elevation suggests pericarditis over OMI. However, you diagnose pericarditis at your (and the patient’s) peril. Pericarditis is relatively rare, with approximately 1/20th the incidence of OMI, so the pretest probability is very low.[13,14] There are multiple ways OMI can present with diffuse ST elevation. It is the clinician’s job to definitively rule out OMI, or other life-threatening conditions, before diagnosing pericarditis.
Anterior and inferior ST elevation together can suggest proximal occlusion of a Type III “wraparound LAD,” which supplies a portion of the inferior wall and may even have anastomosis with the PDA. There will often be lateral ST elevation in patients with proximal LAD occlusion as well. Any ST depression, especially any reciprocal ST depression in aVL, makes the diagnosis of pericarditis unlikely.[15]
Serial ECGs and bedside echocardiogram are valuable in confirming or ruling out OMI in these patients. Dynamic ST changes or wall motion abnormality on echocardiogram confirms coronary occlusion and indicates emergent cardiac catheterization.

Conclusion
Patients presenting with symptoms of ACS must be assumed to have acute coronary artery occlusion until proven otherwise. Assessment can be augmented by performing serial ECGs and bedside echocardiography. The ECG is one of many tools used to diagnose OMI and the astute clinician must be able to recognize ECG signs of OMI that are outside of traditional STEMI guidelines.
References
- Thygesen K, Alpert JS, Jaffe AS, Simoons ML, Chaitman BR, White HD. Third Universal Definition of Myocardial Infarction. Circulation. 2012;126(16):2020-2035.
- Meyers P, Weingart S, Smith S. The OMI Manifesto. Dr Smith’s ECG Blog. 2018.
- Nable JV, Brady W. The evolution of electrocardiographic changes in ST-segment elevation myocardial infarction. Am J Emerg Med. 2009;27(6):734-746.
- Birnbaum Y, Sclarovsky S, Mager A, Strasberg B, Rechavia E. ST segment depression in a VL: a sensitive marker for acute inferior myocardial infarction. Eur Heart J. 1993;14(1):4-7.
- Pollehn T, Brady WJ, Perron AD, Morris F. The electrocardiographic differential diagnosis of ST segment depression. Emerg Med J. 2002;19(2):129-135.
- de Winter RJ, Verouden NJW, Wellens HJJ, Wilde AAM. A New ECG Sign of Proximal LAD Occlusion. N Engl J Med. 2008;359(19):2071-2073.
- Smith SW, Dodd KW, Henry TD, Dvorak DM, Pearce LA. Diagnosis of ST-elevation myocardial infarction in the presence of left bundle branch block with the ST-elevation to S-wave ratio in a modified sgarbossa rule. Ann Emerg Med. 2012;60(6):766-776.
- Sgarbossa EB, Pinski SL, Gates KB, Wagner GS. Early electrocardiographic diagnosis of acute myocardial infarction in the presence of ventricular paced rhythm. GUSTO-I investigators. Am J Cardiol. 1996;77(5):423-424.
- Maloy KR, Bhat R, Davis J, Reed K, Morrissey R. Sgarbossa Criteria are Highly Specific for Acute Myocardial Infarction with Pacemakers. West J Emerg Med. 2010;11(4):354-357.
- van Gorselen EOF, Verheugt FWA, Meursing BTJ, Oude Ophuis AJM. Posterior myocardial infarction: the dark side of the moon. Netherlands Hear J. 2007;15(1):16-21.
- Khan JN, Chauhan A, Mozdiak E, Khan JM, Varma C. Posterior myocardial infarction: are we failing to diagnose this? Emerg Med J. 2012;29(1):15-18.
- Driver BE, Khalil A, Henry T, Kazmi F, Adil A, Smith SW. A new 4-variable formula to differentiate normal variant ST segment elevation in V2-V4 (early repolarization) from subtle left anterior descending coronary occlusion – Adding QRS amplitude of V2 improves the model. J Electrocardiol. 2017;50(5):561-569.
- Awan A, Tiruneh F, Wessly P, et al. Acute Pericarditis: Descriptive Study and Etiology Determination in a Predominantly African American Population. Cureus. 2017;9(7):e1431.
- Sanchis-Gomar F, Perez-Quilis C, Leischik R, Lucia A. Epidemiology of coronary heart disease and acute coronary syndrome. Ann Transl Med. 2016;4(13):256.
- Bischof JE, Worrall C, Thompson P, Marti D, Smith SW. ST depression in lead aVL differentiates inferior ST-elevation myocardial infarction from pericarditis. Am J Emerg Med. 2016;34(2):149-154.