Using POCUS to aid in foreign body causing urinary retention.
A 13-year-old male, otherwise healthy, presented to the emergency department with a chief complaint of difficulty urinating. On further history, the patient admitted to placing a 12-inch rigid plastic string in his urethra 1.5 days prior to presentation. He noted that he had “an itch,” which was the rationale behind the placement of the foreign body. He became concerned when he could no longer urinate but denies penile pain at rest or any penile discharge.
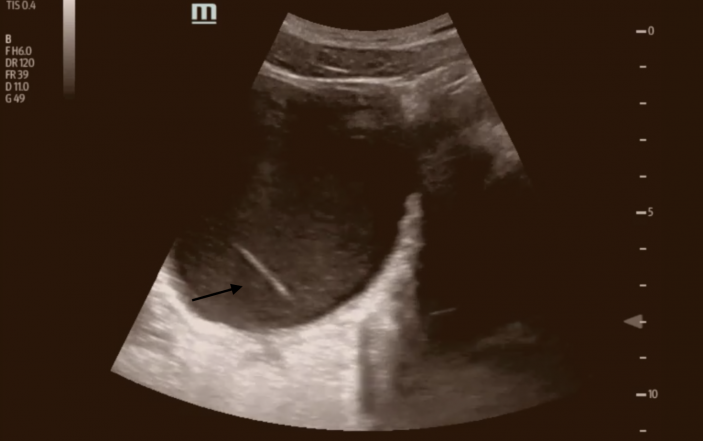
Physical exam was unremarkable including a GU exam, which did not demonstrate any abnormalities. Given concern for migration of the plastic up his urethra, a point of care ultrasound was performed in the ED and demonstrated a foreign body consistent with a plastic string (images 1, 2).


Urology was consulted and the object was removed under general anesthesia. A urine culture obtained in the ED subsequently grew enterococcus and he was treated with a one-week course of antibiotics.
Sexual exploration, efforts at contraception, assault and accidental insertion have all been noted as reasons for genitourinary insertions.[1] In a small case study, 80% of causes of foreign body insertion were iatrogenic.[2] Of those who do seek treatment, hematuria, dysuria, frequency, strangury and retention are the most common presenting complaints.[3] These problems can be exacerbated both by failure to seek care due to embarrassment or attempting to remove the object at home.
Diagnosis is traditionally made by physical exam and clinical history, but depending on location of the object, may require a KUB radiograph or other intensive imaging study.[4] An alternative method is using point-of-care ultrasound.
In our case, point of care ultrasound proved an effective means of identifying the foreign body and negating the need for radiation exposure, which was beneficial given age of patient.
After diagnosis, urology consultation is of vital importance to manage the current injury, and to avoid further injury. Infectious risks and underlying motivations should also not be overlooked in these cases as this behavior can certainly repeat itself.
References
[1] Unruh BT, Nejad SH, Stern TW, Stern TA. Insertion of foreign bodies (polyembolokoilamania): underpinnings and management strategies. Prim Care Companion CNS Disord. 2012;14(1). doi:10.4088/ PCC.11f01192.
[2] Mannan A, Anwar S, Qayyum A, Tasneem RA. Foreign bodies in the urinary bladder and their management: a Pakistani experience. Singapore Medical Journal 2011;52(1):24–8.
[3] Rieder J, Brusky J, Tran V, Stern K, Aboseif S. Review of intentionally self-inflicted, accidental and iatrogenic foreign objects in the genitourinary tract. Urologia Internationalis 2010;84:471–5.
[4] Bedi N, El-Husseiny T, Buchholz N, Masood J. ‘Putting lead in your pencil’: self-insertion of an unusual urethral foreign body for sexual gratification. Journal of the Royal Society of Medicine Short Reports 2010; 1:18.