An ectopic pregnancy after tubal ligation.
Case Report:
A 38-year-old female presented to the emergency department after a positive urine pregnancy test at her primary care physician’s office. Additionally, there were concerns for a possible ectopic pregnancy on a pelvic ultrasound. Upon further questioning, this was her sixth ED visit in the past two days since her initial PCP visit. She mentioned every ED she went to told her the urine pregnancy test was positive, with the most recent serum total beta hCG of 629 one day prior to arrival. The patient noted intermittent vaginal spotting for the past week with associated lower pelvic pain. Her last menstrual period was unknown, but that it could have been at “least two months.” No urine pregnancy test was performed at home as she stated, “There is no way I am pregnant.” Her obstetrical and gynecological history was notable for one prior ectopic pregnancy treated with methotrexate and two prior miscarriages. In addition, she had a bilateral tubal ligation performed about two years ago. Per records, she had undergone a modified Pomeroy technique (bilateral partial salpingectomy).
Vitals on arrival to the ED: 98.7 °F, blood pressure of 121/78 mmHg, heart rate of 73 beats/min, respiratory rate of 13 breaths/min, 72 kg, and a pulse ox of 99% on room air. On physical exam, the patient appeared frustrated and angry. Her abdominal exam revealed minimal left lower adnexal tenderness with no peritoneal signs. A subsequent urine pregnancy test was positive in the ED and a total serum beta hCG resulted at 744.
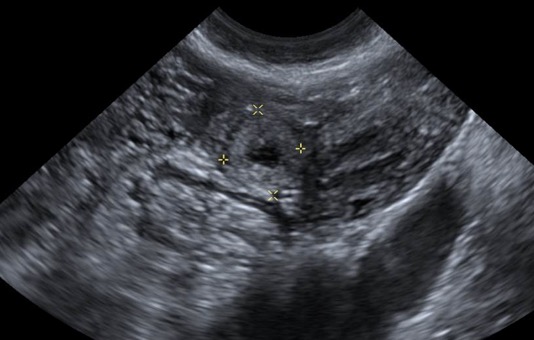
A transvaginal ultrasound, image A, showed a thick walled complex cystic structure measuring up to 1.0 cm within the left adnexa. Per the radiology report, it was difficult to ascertain whether this arose from the left ovary or if it was separate from the left ovary. In light of the patient’s total serum beta hCG, an ectopic pregnancy could not be excluded. After a lengthy discussion with the patient, she agreed to be evaluated in the ED by obstetrics and gynecology and a diagnostic laparoscopy was recommended. She consented and was taken to the operating room. Upon entry into the abdomen about 25 cc of hemoperitoneum was encountered within the pelvis. The uterus was approximately eight weeks in size. The left ovary appeared normal. The left/right fallopian tubes were consistent with a history of a bilateral tubal ligation. There was an area of distention noted (1×2 cm) distal to the site of the previous modified Pomeroy with blood clots at the fimbriated end of the left tube. The patient subsequently underwent a left salpingectomy and removal of the ectopic pregnancy. Her remaining hospital course was unremarkable, and she was discharged on day 2.

Discussion:
An ectopic pregnancy is a potentially fatal obstetrics and gynecological emergency. The prevalence is roughly about 2% within the general population. However, in patients presenting to the ED with vaginal bleeding during the first trimester, it increases up to 16%.[1] Without quick recognition, the patient can rapidly decompensate leading to hemorrhagic shock and death when rupture occurs. Within the first trimester, an ectopic pregnancy becomes the leading cause of maternal mortality.[2]
Risk factors include, but not limited to:
- History of pelvic inflammatory disease
- Prior ectopic pregnancy
- Intrauterine device
- Prior tubal surgery
- Multiple sexual partners
- In vitro fertilization
- Cigarette smoking
- Prior abortion(s).
It should be noted that within the literature, 50% of patients with an ectopic pregnancy are often asymptomatic prior to rupture and present to the ED with no identifiable risk factors.[3] While no single presenting sign/symptom is pathognomonic of an ectopic pregnancy, patients can present without symptoms, just vaginal bleeding/pelvic pain in a non-ruptured ectopic pregnancy, to massive intraperitoneal hemorrhage and shock when rupture occurs.
Conclusion:
We have all heard our patients say, “There is no way I am pregnant, I had my tubes tied.” What is the incidence of an ectopic pregnancy in this patient population? The particular tubal ligation our patient had is called a modified Pomeroy procedure, the most commonly used method for sterilization.4 This was performed at an outside institution approximately two years prior to our patient’s presentation.
One systematic review utilizing the Cochrane database, data from MEDLINE, and observational studies found that the Pomeroy procedure showed no difference in failure rates between one of the next most common sterilization procedures, the application of mechanical devices like Filshie clips.4 The modified Pomeroy technique involves making cuts at the end of the fallopian tubes and leaving a gap of 3-4 cm. The suture material eventually reabsorbs, and the peritoneum eventually grows over to cover the tubal ends.[4]
Partial salpingectomy utilizing the modified Pomeroy technique for sterilization carries with it a failure rate of 7.5 per 1,000 surgeries, (6/1,000 for other procedures), with an ectopic pregnancy rate of 1.5 per 1,000 surgeries, likely related to fistula formation.[4] In the ED setting, unless the patient has a documented history of a total abdominal hysterectomy, pregnancy should still be considered in any female patient presenting with pelvic pain, even if they have had a tubal ligation.
References:
- Robertson, J, Koyfman, A. “Ectopic Pregnancy.” emDOCS. http://www.emdocs.net/ectopic-pregnancy/
- Tulandi, T, “Incidence, risk factors, and pathology of ectopic pregnancy.” UpToDate, October 2013. https://uptodate.yhdp.vn/contents/UTD.htm?21/15/21752/abstract/31,33
- Tulandi, T, “Ectopic pregnancy: Clinical manifestations and diagnosis.” UpToDate, May 2, 2017. https://www.uptodate.com/contents/ectopic-pregnancy-clinical-manifestations-and-diagnosis
- Madari, S, Varma, R, Gupta, J. “A comparison of the modified Pomeroy tubal ligation and Filshie clips for immediate postpartum sterilization. A systematic review.” European Journal of Contraception and Reproductive Health Care. 2011 Oct;16(5):341-9. https://www.ncbi.nlm.nih.gov/pubmed/21929362