The emergency department (ED) is not an ideal place for patients with depression to seek help. Waiting times, busy staff, and a greater likelihood of a fleeting interaction with a physician coincide with the reality that many emergency physicians do not receive training for depression screening.
Yes: EPs should screen for depression and begin treatment
by Lonnie Stoltzfoos with David Hoyer, MD
The emergency department (ED) is not an ideal place for patients with depression to seek help. Waiting times, busy staff, and a greater likelihood of a fleeting interaction with a physician coincide with the reality that many emergency physicians do not receive training for depression screening.
“By and large, patients don’t typically come into the ED saying ‘I’m depressed and I need help.’
Instead, many patients complain of depression’s symptoms, like trouble sleeping” says Dr. David Hoyer. “If the emergency physician is not familiar with screening for depression, the patient may get an incomplete evaluation and then be discharged from the ED with a diagnosis that does not fully represent the problems that the patient is having.”
 Several studies, including one of Dr. Hoyer’s, show that prevalence rates of depression in ED patients may range from 20%–30%. Dr. Hoyer therefore advocates quick, simple depression screening in the ED when adult patients present with depressed affect, vague complaints, and/or there is a uniformly positive review of systems.
Several studies, including one of Dr. Hoyer’s, show that prevalence rates of depression in ED patients may range from 20%–30%. Dr. Hoyer therefore advocates quick, simple depression screening in the ED when adult patients present with depressed affect, vague complaints, and/or there is a uniformly positive review of systems.
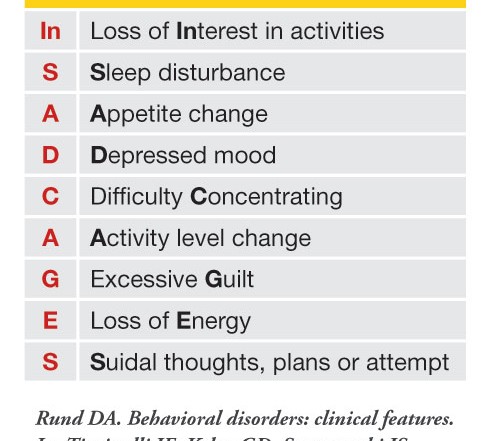
Most screens for depression were developed by psychiatrists or researchers and are impractical for the bedside use of emergency physicians. When seeing patients he suspects may be depressed, Dr. Hoyer prefers the check list “In SAD CAGES” developed by Dr. Doug Rund, an emergency physician (Table). To screen positive for depression, the patient must have at least 5 of the 9 criteria on a daily basis for at least 2 weeks, including either loss of interest in activities or depressed mood.
“If you’re a busy emergency physician, screening with ‘In SAD CAGES,’ which takes 30 seconds to 2 minutes, may be all the time you can allot to the consideration of depression in a patient,” says Dr. Hoyer.
That emergency physicians have precious little time to devote to patients is not disputed. The debate revolves around not only whether emergency physicians ought to screen their patients for depression in the first place, but also around what exactly they should do with patients who screen positive for depression. Dr. Hoyer believes firmly that emergency physicians should consider initiating antidepressant treatment (such as fluoxetine) for ED patients, a practice he has followed for the past 20 years.
“After I screen someone and rule out other potential causes of the patient’s symptoms, thereby arriving at a tentative diagnosis of depression, I think it is in the patient’s best interest to consider initiating an antidepressant (unless they are suicidal, psychotic, or manic, which would necessitate a psychiatric consultation),” says Dr. Hoyer. “People with depression may have diminished motivation to seek help, but if you make a tentative diagnosis in the ED and give them a prescription, there is a greater likelihood that the patient will follow up on a referral for further care. Many people receive early benefits from antidepressants, and by the time they go for follow-up in 7–10 days they may already be improving.
“Of course, I am an exception to the status quo,” continues Dr. Hoyer, “and this issue goes back to training and experience—if you haven’t been trained to evaluate for psychiatric problems then you certainly won’t prescribe a medication for those problems. Emergency medicine is still a new specialty, however, so there are emergency physicians who were trained in different specialties, especially family medicine. (Family doctors prescribe the majority of antidepressants in the US today.) Still other emergency physicians might feel comfortable restarting antidepressants for patients with past depressive episodes treated with an antidepressant.”
Dr. Hoyer encourages emergency physicians who are not comfortable initiating medication to at least become familiar with screening for depression using “In SAD CAGES.” Many patients suspect that they are depressed and are grateful to know they can seek help when an emergency physician informs them that they meet the criteria for depression. Patients who screen positive could be discharged from the ED with a diagnosis of depression as long as they are not suicidal and have a reasonable follow-up plan.
“In terms of the evidence base, this subject is still greatly under-discussed and under-researched,” concludes Dr. Hoyer. “There is a great need for research on the best way to deal with depression in the ED. Meanwhile, depression has a known morbidity and mortality, and we owe it to our patients to at least screen those at risk for this disease.”
No: Messing with SSRIs without confirmed follow-up can do more harm than good
by Kevin Klauer, DO, EJD
Although there are substantial issues with access to mental health services for emergency department patients that present with psychiatric complaints, it doesn’t mean that emergency physicians should take on the role of counselor, therapist or psychiatrist. And it certainly does not mean that we should start prescribing antidepressants in the ED.
The problem is that emergency physicians have been conditioned over the years to accept the word “No” from other providors and move on with the only solution we think we can truly count on: ourselves. But when we self-delegate every task and issue that others deflect to us, it enables others to avoid their responsibilities. And in the end, care suffers.
Focusing on the issue of depression, what is the issue? We know that patients with depression present to the ED every day (and even more get depressed because of being in the ED, including the staff). We also know that most issues with access to mental health services are compensation-based. If our patients don’t have insurance, they often cannot obtain services. But just because ED patients have access issues with psychiatrists, does that mean the EPs should be ordering SSRIs? Do SSRIs impact the major concern of EPs, namely suicide?
So, in lieu of finding creative ways to improve access, what are the solutions? I certainly don’t espouse to know the answers, but I know that adding bad solutions on top of bad problems only makes things worse.
Some emergency physicians propose that we take on yet another responsibility that isn’t ours, initiating antidepressants in the emergency department. I suppose it may seem altruistic and appropriate to start whatever management is necessary and refer our patients for follow up and ongoing management. However, depression is a bit different. First, can we ensure appropriate follow-up will occur? If we could, then perhaps we wouldn’t have a pressing need to start these medications in the ED.
Second, will this improve care? We all want to fix what is broken. However, mental health is not like other pathology we treat. I submit that there are a good number of patients who are depressed that are not significantly benefited by the use of antidepressants. On January 4th, 2012, the Chicago Tribune reported that the FDA has noted that of the 30 million Americans who take antidepressants, only 30% respond to the first agent prescribed. Thus, nearly a third will require an alternative agent or additional medications.
We also have to consider that some portion of that 30% are just plain goofy (no neurotransmitter imbalance) and won’t respond to anything at all.
Third, is it safe? Some may say, particularly with serotonin reuptake inhibitors (SSRIs), “What’s the harm? These drugs are prescribed like candy, and they’re really safe.” Not so fast! There is another side to this story that must be told. There is an age-dependent (predominantly 25 years and younger) association with increased suicidality and suicide attempts with the use of these medications and that risk is noted primarily in the initial weeks of treatment. A meta-analysis from McGill University reviewed 702 randomized, controlled trials: SSRIs vs. placebo or non-SSRIs. Over 87,000 patients were studied. 345 studies reported 36,445 suicide attempts. The odds ratio for an attempt, when compared to placebo was 2.28, over twice as likely (Fergusson, D., et al, Br Med J 330:396, February 19, 2005). Safe? I doubt it.
The altruistic DNA of emergency physicians compels us to do whatever it takes to help whomever we can. When faced with broken, we must fix. However, there are circumstances in which tinkering with that which has traditionally been handled in other settings may cause real trouble. Perhaps, messing with neurotransmitters without confirmed follow up with a psychiatrist should be off limits.
4 Comments
From my perspective, if a patient has significant enough symptoms whether by “IN-SAD-CAGES” evaluation, history or just plain gestalt such that I feel they would benefit from antidepressants, then THAT patient is at risk in my opinion. Nothing less than a baseline medical screening evaluation to look for subtle organic causes (like hypothyroidism for example)followed by evaluation by a Psychiatric team member is going to meet the patient’s needs. If these options are not available, and the patient is willing, then ED observation until appropriate followup can be arranged. We all know SSRI’s are certainly not without side effect and/or risks. So why should I as the EP who see’s them for a mere screenshot in the film of their lives be the one to begin such non-innocuous therapy? Woefully illogical and misguided thinking! This whole thing reeks of more “sweeping problems under the rug at ambulance triage door in the ED”. Such “band-aid fixes” simply overload the “health care safety net” even more. The answer is no. The appropriate people should prescribe AND follow these patients so they can be managed correctly. But of course, since patients are held to no particular standard, whatever we do will only be at most 50% effective, depending on how compliant they themselves are.
Given that the effect of SSRI vs placebo is virtually identical and the myriad of adverse effects SSRI’s can cause this is foolish. Those advocating this should declare their conflicts as this smells of pharma propaganda.
Psychiatrists are so arrogant.
They possess “special knowledge” which makes them singularly able to help the “mentally ill.” Oh, but yeah…go ahead and let the emergency room doctor diagnose mental illness, too. I mean, why not? The psychs developed programs which allow teachers and school personnel to “identify” kids with ADHD.
So really, how special is psychiatric knowledge?
How much training does it take to label someone with depression or whatever?
Not much. You just have to be devoid of compassion for your fellow human being and have no clue that all “mental symptoms” have a physically-based etiology.
All mental manifestations can be cured or alleviated by addressing physical causes. But then psychiatrists wouldn’t make nearly as much money, would they?
You EPs are killing people!
Of course you prescribe SSRIs in the ED. Saying otherwise would be like saying that you shouldn’t prescribe amoxicillin in the ED, because patients need appropriate follow up with their PCP, just in case.
The British Journal of Psychiatry (2018) 212, 148–154. doi: 10.1192/bjp.2017.24