
Case:
A 33-year-old male presented to the emergency department for hemoptysis for two days. The patient reported periods of coughing up blood-streaked sputum, generalized fatigue, and orthopnea. He denied chest pain. He had a history of nonischemic cardiomyopathy (NICM) with an ejection fraction of 15% which was diagnosed a month prior to this visit during a hospital admission for cardiogenic shock.
An echocardiogram at that time showed multiple large LV and RV thrombi (figures 1a-c).
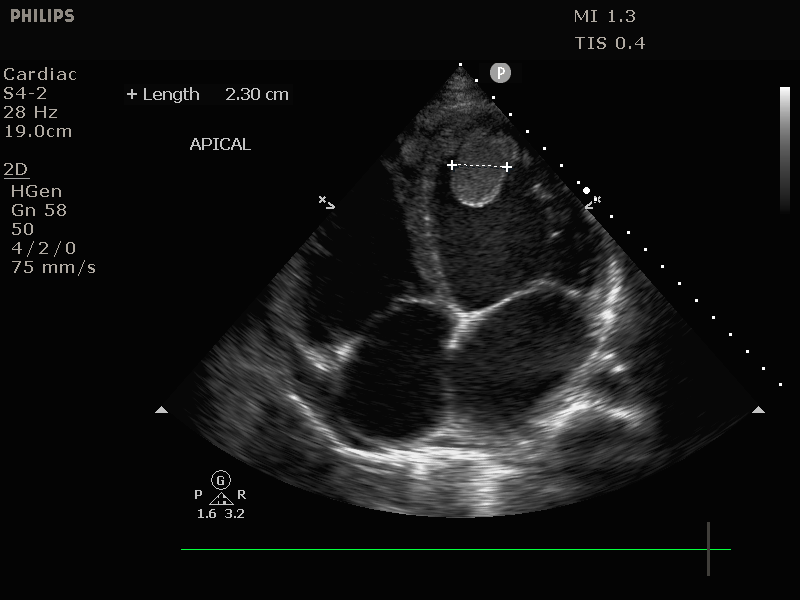
Apical thrombus : 4 chamber view of the heart showing a 2.3cm thrombus adhering to the cardiac apex;
The patient was started on Eliquis during that admission, and he reported no missed doses since discharge. The etiology of these thrombi was thought to be due to the patient’s use of methamphetamines. Notably, the patient’s father also had a history of cardiomyopathy which was diagnosed in his 30s.
On exam, the patient appeared ill. He was hypotensive with a blood pressure of 92/62 and tachycardic at 105 bpm. He was afebrile and saturating appropriately on room air. Lungs were clear to auscultation bilaterally and cardiac exam was positive for an S3 gallop. JVP was elevated. He had cool distal extremities and normal distal pulses. There were no lower extremity edema or skin changes. The remainder of the exam was unremarkable.
EKG showed sinus rhythm with a 1st degree AV block. Labs were notable for an elevated lactate of 2.9 which up-trended to 3.6. Hemoglobin was stable. Given concern for cardiogenic shock, norepinephrine was started. A CXR demonstrated cardiomegaly and batwing perihilar opacities consistent with pulmonary edema (figure 2).

CXR showing cardiomegaly with severe bilateral pulmonary edema.
CTA chest was negative for PE but did show severe global cardiomegaly and diffuse ground glass opacities consistent with pulmonary edema (figure 3).
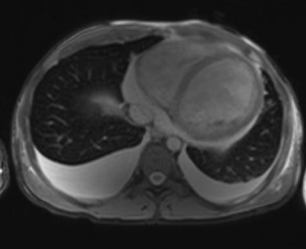
Chest CT showing cardiomegaly with bilateral pleural effusions.
Bedside echocardiogram was notable for enlargement of all four chambers and severely reduced LV and RV function (figure 4).

Apical four chamber view on bedside echocardiogram during end diastole showing dilated left ventricle with decreased excursion of the mitral valve.
Subcostal view of the IVC on bedside echocardiogram showing >2cm of dilation with minimal respiratory variability (figure 5).

Subcostal view of the IVC on bedside echocardiogram showing >2cm of dilation with minimal respiratory variability.
The patient was admitted to the cardiac ICU for further evaluation and treatment.
During his admission, he was started on dobutamine for inotropic support. Nitroprusside and valsartan were started for afterload reduction without any improvement. He was unable to be weaned from dobutamine. Repeat echocardiogram was notable for worsening of the patient’s EF to 10% and resolution of the previously identified LV and RV thrombi. LHC showed non-obstructive disease. He was transferred to another hospital for potential LVAD and transplant evaluation given concern for inotropic failure but was unable to undergo invasive treatment given ongoing methamphetamine use.
At the tertiary care hospital, he was continued on dobutamine for ionotropic support as well as nitroprusside. Repeat ECHO showed an EF of 10% with a low cardiac output state. A left catheterization demonstrated non-obstructive disease, but the left circumflex artery had an 80% tubular lesion which may have been thrombotic in origin. He was ultimately weaned off his infusions and transferred to a cardiac floor. A heart failure team felt that he was not a candidate for advanced therapies. He was discharge with guideline directed medical therapy and outpatient follow up.
Discussion:
Nonischemic cardiomyopathy occurs when a patient’s cardiomyopathy is not caused by coronary artery disease. A common cause of NICM is substance induced, with cocaine being a well-recognized as having cardiotoxic effects. (1) Another substance that can cause of NICM is methamphetamines, such as in this patient.
Methamphetamines can have significant effects on the cardiorespiratory system, causing vasoconstriction, pulmonary artery hypertension, atherosclerotic plaques, arrhythmias, and cardiomyopathy. Methamphetamine works by promoting catecholamine release in the bloodstream. Cardiovascular disease is second only to overdose for the leading cause of death of methamphetamine users. (2)
Methamphetamine causes a rapid increase in both heart rate and blood pressure, ultimately causing vasoconstriction. Acutely, this can cause acute angina due to vasospasm of the coronary arteries. Chronically, methamphetamine use can result in pulmonary arterial hypertension. In the lungs it is primarily metabolized by pulmonary endothelial cells, ultimately enhancing apoptosis. (3)
A known downstream effect of chronic methamphetamine use is a dilated cardiomyopathy. This mechanism is multifactorial, likely involving excess catecholamines, reactive oxygen species, mitochondrial dysfunction, vasospasm and ischemia. (4)
Cardiogenic shock occurs when tissue perfusion is limited due to poor cardiac output causing poor forward blood flow from the heart and carries a high mortality rate. The mainstays of management for cardiogenic shock include volume management via diuretics, but also inotropic support to promote forward blood flow. Inotropes such as dobutamine, dopamine, epinephrine and norepinephrine ultimately increase myocardial contractility through increasing intracellular calcium concentrations.
In the emergency department, norepinephrine is often the first vasopressor of choice due to its inotropic and vasoconstrictive properties. Following this, dobutamine can be used for its inotropic properties. Dobutamine usage must be monitored because its effects on mean arterial pressure can vary. Both norepinephrine and dobutamine can be used in conjunction for inotropic support. If inotropic support fails, additional evaluation may be needed for mechanical assistance for cardiogenic shock via a device such as a left ventricular assist device (LVAD). (5)
Resources:
- https://www.nature.com/articles/s41598-020-76273-1.pdf
- https://pubmed.ncbi.nlm.nih.gov/28787694/
- https://www.ahajournals.org/doi/epub/10.1161/ATVBAHA.119.312461
- https://pubmed.ncbi.nlm.nih.gov/24037954/
- https://onlinelibrary.wiley.com/doi/epdf/10.1002/ejhf.3162
Photo Credit: www.kaboompics.com